Você também pode gostar
- Paranasal Sinus Cancer A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandParanasal Sinus Cancer A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- Ludwig AnginaDocumento7 páginasLudwig AnginaCak BasitAinda não há avaliações
- Deep Neck Infection1deep Neck Space InfectionDocumento53 páginasDeep Neck Infection1deep Neck Space Infectionwhitelotusoo7Ainda não há avaliações
- Deep Neck Space InfectionDocumento48 páginasDeep Neck Space InfectionhaneiyahAinda não há avaliações
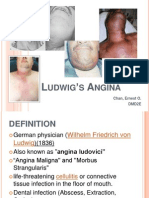
- Ludwig's AnginaDocumento9 páginasLudwig's AnginaErnest Chan0% (1)
- Tracheostomy: Presented By: Barte, Hannah Aida D. Balamurugan, RameebhaDocumento21 páginasTracheostomy: Presented By: Barte, Hannah Aida D. Balamurugan, RameebhaThakoon Tts100% (1)
- Inguinal Hernias: CaseDocumento6 páginasInguinal Hernias: Casechomz14Ainda não há avaliações
- Deep Neck Infection 051005Documento43 páginasDeep Neck Infection 051005Vishal GauravAinda não há avaliações
- Deep Neck Space InfectionsDocumento43 páginasDeep Neck Space InfectionsmariscaclaudiaaAinda não há avaliações
- By Abayneh Ayele (Ieso Student) Wollo UniversityDocumento68 páginasBy Abayneh Ayele (Ieso Student) Wollo UniversitydenekeAinda não há avaliações
- PneumothoraxDocumento43 páginasPneumothoraxSravani KanchiAinda não há avaliações
- TracheostomyDocumento3 páginasTracheostomySarah Elizabeth WalkerAinda não há avaliações
- Hospital Acquired PneumoniaDocumento21 páginasHospital Acquired PneumoniaNatashaDianasari100% (1)
- HEMATOCHEZIADocumento26 páginasHEMATOCHEZIAAlvin HartantoAinda não há avaliações
- Chest Tube DrainageDocumento45 páginasChest Tube DrainageDonald BidenAinda não há avaliações
- Kaposi SarcomaDocumento41 páginasKaposi SarcomaMihaela Pal0% (1)
- 14 OtosclerosisDocumento76 páginas14 OtosclerosisAatif_Saif_80Ainda não há avaliações
- PeritonitisDocumento19 páginasPeritonitisAditya SahidAinda não há avaliações
- EMPYEMADocumento27 páginasEMPYEMAMark Bin S. DilangalenAinda não há avaliações
- Gastrointestinal Fistula: DR Vihar Kotecha M.D, M.MED Gen Surg (Nbi), FCS Gen Surg (ECSA) Lecturer CUHASDocumento60 páginasGastrointestinal Fistula: DR Vihar Kotecha M.D, M.MED Gen Surg (Nbi), FCS Gen Surg (ECSA) Lecturer CUHASSangija kamataAinda não há avaliações
- Chronic Tonsillitis PDFDocumento27 páginasChronic Tonsillitis PDFAnanta Ayu WulansariAinda não há avaliações
- Sialadenitis: K.Abhinaya. Bds 3 YearDocumento14 páginasSialadenitis: K.Abhinaya. Bds 3 YearAsline JesicaAinda não há avaliações
- HerniaDocumento36 páginasHerniashankarrao3Ainda não há avaliações
- Acute CholecystitisDocumento28 páginasAcute CholecystitisWilfredo Mata JrAinda não há avaliações
- Inverted Papilloma Nose and Its ManagementDocumento20 páginasInverted Papilloma Nose and Its ManagementDr. T. Balasubramanian100% (3)
- Cholecystitis Cholelithiasis PresentationDocumento21 páginasCholecystitis Cholelithiasis PresentationPrincess Meinny JeanAinda não há avaliações
- TracheostomyDocumento29 páginasTracheostomyFemi AustinAinda não há avaliações
- Bowel ObstructionDocumento48 páginasBowel ObstructionItHa Sagiitariius BLue LoverzAinda não há avaliações
- Anatomy of Deep Neck Spaces - SentyDocumento18 páginasAnatomy of Deep Neck Spaces - SentySenti AnnamalaiAinda não há avaliações
- Chronic TonsillitisDocumento47 páginasChronic Tonsillitissuci0% (1)
- Respiratory System DisordersDocumento9 páginasRespiratory System Disordersasop06Ainda não há avaliações
- 01 Enteral and Parenteral Nutrition Support PSIK UMMDocumento68 páginas01 Enteral and Parenteral Nutrition Support PSIK UMMSri YulianaAinda não há avaliações
- CHOLEDOCHOLITHIASISDocumento38 páginasCHOLEDOCHOLITHIASISPrecious Cofreros100% (3)
- Pancreatitis: Dr. Ahmad Aqel RN, PHD The University of Jordan 2015Documento27 páginasPancreatitis: Dr. Ahmad Aqel RN, PHD The University of Jordan 2015Anonymous 5HzElnmAinda não há avaliações
- Cholecystitis Cholelithiasis PresentationDocumento21 páginasCholecystitis Cholelithiasis PresentationDe WiqAinda não há avaliações
- Bowel PreparationDocumento16 páginasBowel PreparationKateAngeliRebosuraAinda não há avaliações
- Inflammatory Bowel DiseaseDocumento14 páginasInflammatory Bowel Diseasehazelel100% (1)
- Chest TubeDocumento8 páginasChest TubeTaufik Nur YahyaAinda não há avaliações
- Penetrating Chest Trauma With Massive Hemothorax by A Small StoneDocumento2 páginasPenetrating Chest Trauma With Massive Hemothorax by A Small Stoneputri firda erlinaAinda não há avaliações
- Tracheostomy: Dr. Amar KumarDocumento18 páginasTracheostomy: Dr. Amar KumarSudhanshu ShekharAinda não há avaliações
- Total Penectomy Urooncology 12thDocumento10 páginasTotal Penectomy Urooncology 12thdr. Joko WibowoAinda não há avaliações
- Deep Neck Space InfectionsDocumento77 páginasDeep Neck Space InfectionsKIBET ERNEST MUTAIAinda não há avaliações
- HerniaDocumento16 páginasHerniaVetrivel TamizhAinda não há avaliações
- TracheostomyDocumento31 páginasTracheostomyTonyScaria100% (1)
- Ventilator Associated Infections VENTILATOR ASSOCIATED PNEUMONIA - CARE AND PREVENTIONDocumento102 páginasVentilator Associated Infections VENTILATOR ASSOCIATED PNEUMONIA - CARE AND PREVENTIONtummalapalli venkateswara raoAinda não há avaliações
- Enterocutaneous FistulaDocumento34 páginasEnterocutaneous FistulaAkram ChalidAinda não há avaliações
- Wound de His Cence FinalDocumento26 páginasWound de His Cence Finaldanil armandAinda não há avaliações
- Stoma ComplicationsDocumento35 páginasStoma ComplicationsAlex Ciorogar100% (1)
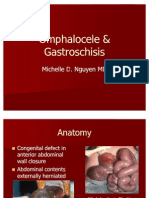
- Omphalocele GastroschisisDocumento12 páginasOmphalocele GastroschisisOlivelhynn Bernaldo100% (1)
- CHOLEDOCHOLITHIASISDocumento8 páginasCHOLEDOCHOLITHIASISkuncupcupu1368Ainda não há avaliações
- Rectal ProlapseDocumento29 páginasRectal ProlapseErick AkwanAinda não há avaliações
- EpistaxisDocumento33 páginasEpistaxispaulyn ramosAinda não há avaliações
- Cholecystitis & Carcinoma of GallbladderDocumento37 páginasCholecystitis & Carcinoma of GallbladderSalsabila Al-Basheer100% (1)
- PeritonitisDocumento34 páginasPeritonitisabrar_zaidiAinda não há avaliações
- Oral ThrushDocumento29 páginasOral ThrushTushar KhuranaAinda não há avaliações
- Cleft Lip and PalateDocumento14 páginasCleft Lip and PalateMin100% (1)
- Diseases of Respiratory SystemDocumento23 páginasDiseases of Respiratory SystemMarchelle Fae EsmallaAinda não há avaliações
- Airway ObstructionDocumento32 páginasAirway ObstructionAmirrah LaurenteAinda não há avaliações
- RESTRICTIVE LUNG DISEASES (Autosaved)Documento40 páginasRESTRICTIVE LUNG DISEASES (Autosaved)Dr. Rabail MalikAinda não há avaliações
- Ludwig AnginaDocumento5 páginasLudwig AnginaSiti Aprilia wahyuniAinda não há avaliações
- Distribution Channel - PackagingDocumento10 páginasDistribution Channel - PackagingDevavrat SinghAinda não há avaliações
- Standard Operating Procedures in Pharmaceutical IndustryDocumento38 páginasStandard Operating Procedures in Pharmaceutical IndustryDevavrat Singh25% (4)
- Distribution Channel - Performance MetricsDocumento18 páginasDistribution Channel - Performance MetricsDevavrat SinghAinda não há avaliações
- Service Chain: by Amardeep Ukrande Amrita Tripathi Apurva Kulkarni Rucha Vaidya Yashasvi SanghaviDocumento28 páginasService Chain: by Amardeep Ukrande Amrita Tripathi Apurva Kulkarni Rucha Vaidya Yashasvi SanghaviDevavrat SinghAinda não há avaliações
- Logistics: Tejaswini Babbepall (12) Arjun Saluja (22) Rachna Shah (8) Nidhi Sarda (7) Shiva DhawanDocumento43 páginasLogistics: Tejaswini Babbepall (12) Arjun Saluja (22) Rachna Shah (8) Nidhi Sarda (7) Shiva DhawanDevavrat SinghAinda não há avaliações
- Hero Honda SplitDocumento23 páginasHero Honda SplitDevavrat SinghAinda não há avaliações
- Advertising Effectiveness: Why Sales Can't Be The Only Measure?Documento8 páginasAdvertising Effectiveness: Why Sales Can't Be The Only Measure?Devavrat SinghAinda não há avaliações
- Learningtableau Setpbystep 150107130818 Conversion Gate01Documento108 páginasLearningtableau Setpbystep 150107130818 Conversion Gate01Girishkumar Kaisetty100% (5)
- Reasons Why The Facebook IPO FailedDocumento9 páginasReasons Why The Facebook IPO FailedDevavrat SinghAinda não há avaliações
- Customer Relationship Management-2Documento65 páginasCustomer Relationship Management-2Devavrat Singh100% (1)
- Formal Letter Collaboration TemplateDocumento1 páginaFormal Letter Collaboration TemplateDevavrat SinghAinda não há avaliações
- MDI GDPI Prep - StrategyDocumento10 páginasMDI GDPI Prep - StrategyDevavrat SinghAinda não há avaliações
- Transforming Leadership - Twelve O'clock HighDocumento16 páginasTransforming Leadership - Twelve O'clock HighDevavrat SinghAinda não há avaliações
- TESTDocumento27 páginasTESTLegal CheekAinda não há avaliações
- CSE 202.04 Inspection of Concrete StructuresDocumento67 páginasCSE 202.04 Inspection of Concrete StructuresJellyn BaseAinda não há avaliações
- Research 093502Documento8 páginasResearch 093502Chrlszjhon Sales SuguitanAinda não há avaliações
- 19c Upgrade Oracle Database Manually From 12C To 19CDocumento26 páginas19c Upgrade Oracle Database Manually From 12C To 19Cjanmarkowski23Ainda não há avaliações
- EKC 202ABC ManualDocumento16 páginasEKC 202ABC ManualJose CencičAinda não há avaliações
- Project Formulation and Appraisalpdf PDFDocumento12 páginasProject Formulation and Appraisalpdf PDFabhijeet varadeAinda não há avaliações
- Production of Bioethanol From Empty Fruit Bunch (Efb) of Oil PalmDocumento26 páginasProduction of Bioethanol From Empty Fruit Bunch (Efb) of Oil PalmcelestavionaAinda não há avaliações
- Current Concepts in Elbow Fracture Dislocation: Adam C Watts, Jagwant Singh, Michael Elvey and Zaid HamoodiDocumento8 páginasCurrent Concepts in Elbow Fracture Dislocation: Adam C Watts, Jagwant Singh, Michael Elvey and Zaid HamoodiJoão Artur BonadimanAinda não há avaliações
- National Football League FRC 2000 Sol SRGBDocumento33 páginasNational Football League FRC 2000 Sol SRGBMick StukesAinda não há avaliações
- Aakriti 1Documento92 páginasAakriti 1raghav bansalAinda não há avaliações
- Regional Manager Business Development in Atlanta GA Resume Jay GriffithDocumento2 páginasRegional Manager Business Development in Atlanta GA Resume Jay GriffithJayGriffithAinda não há avaliações
- Blockchains: Architecture, Design and Use CasesDocumento26 páginasBlockchains: Architecture, Design and Use Caseseira kAinda não há avaliações
- Expression of Interest (Consultancy) (BDC)Documento4 páginasExpression of Interest (Consultancy) (BDC)Brave zizAinda não há avaliações
- Colorfastness of Zippers To Light: Standard Test Method ForDocumento2 páginasColorfastness of Zippers To Light: Standard Test Method ForShaker QaidiAinda não há avaliações
- 788 ManualDocumento16 páginas788 Manualn0rdAinda não há avaliações
- Asterisk NowDocumento82 páginasAsterisk Nowkambojk100% (1)
- Эквивалентная Схема Мотра Теслы с Thomas2020Documento7 páginasЭквивалентная Схема Мотра Теслы с Thomas2020Алексей ЯмаAinda não há avaliações
- Standard Test Methods For Rheological Properties of Non-Newtonian Materials by Rotational (Brookfield Type) ViscometerDocumento8 páginasStandard Test Methods For Rheological Properties of Non-Newtonian Materials by Rotational (Brookfield Type) ViscometerRodrigo LopezAinda não há avaliações
- Prospekt Puk U5 en Mail 1185Documento8 páginasProspekt Puk U5 en Mail 1185sakthivelAinda não há avaliações
- BLP#1 - Assessment of Community Initiative (3 Files Merged)Documento10 páginasBLP#1 - Assessment of Community Initiative (3 Files Merged)John Gladhimer CanlasAinda não há avaliações
- Case Study - Kelompok 2Documento5 páginasCase Study - Kelompok 2elida wenAinda não há avaliações
- Derebe TekesteDocumento75 páginasDerebe TekesteAbinet AdemaAinda não há avaliações
- Application of Geoelectric Method For GroundwaterDocumento11 páginasApplication of Geoelectric Method For GroundwaterMunther DhahirAinda não há avaliações
- P 348Documento196 páginasP 348a123456978Ainda não há avaliações
- EKRP311 Vc-Jun2022Documento3 páginasEKRP311 Vc-Jun2022dfmosesi78Ainda não há avaliações
- Previous Year Questions - Macro Economics - XIIDocumento16 páginasPrevious Year Questions - Macro Economics - XIIRituraj VermaAinda não há avaliações
- Wwii TictactoeDocumento2 páginasWwii Tictactoeapi-557780348Ainda não há avaliações
- Surgery - 2020 With CorrectionDocumento70 páginasSurgery - 2020 With CorrectionBaraa KassisAinda não há avaliações
- Agency Canvas Ing PresentationDocumento27 páginasAgency Canvas Ing Presentationkhushi jaiswalAinda não há avaliações
- Chapter 4 - Basic ProbabilityDocumento37 páginasChapter 4 - Basic Probabilitynadya shafirahAinda não há avaliações