Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Nurse's Role and Responsibilities in Administration of MedicationDocumento88 páginasNurse's Role and Responsibilities in Administration of MedicationSonia Singh88% (33)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- QUICK GUIDE – Morpheus8 Treatment ParametersDocumento2 páginasQUICK GUIDE – Morpheus8 Treatment ParametersJW100% (3)
- Teach ManualDocumento78 páginasTeach ManualShouvik DebnathAinda não há avaliações
- Benefits and Risks of Antiretroviral TherapyDocumento12 páginasBenefits and Risks of Antiretroviral TherapyAtgy Dhita AnggraeniAinda não há avaliações
- Referat Obgyn FixDocumento29 páginasReferat Obgyn FixDexter BluesAinda não há avaliações
- Activation of mTOR: A Culprit of Alzheimer's Disease?: Neuropsychiatric Disease and Treatment DoveDocumento16 páginasActivation of mTOR: A Culprit of Alzheimer's Disease?: Neuropsychiatric Disease and Treatment Dovemr dexterAinda não há avaliações
- Ulkus Kornea Eng VerDocumento15 páginasUlkus Kornea Eng VerDexter BluesAinda não há avaliações
- QuestionsDocumento1 páginaQuestionsDexter BluesAinda não há avaliações
- Medi 96 E5795 PDFDocumento5 páginasMedi 96 E5795 PDFDexter BluesAinda não há avaliações
- Pamj 24 182 PDFDocumento5 páginasPamj 24 182 PDFDexter BluesAinda não há avaliações
- Nejmoa1514762 PDFDocumento12 páginasNejmoa1514762 PDFDexter BluesAinda não há avaliações
- SDJ 2016 09 01 PDFDocumento7 páginasSDJ 2016 09 01 PDFDexter BluesAinda não há avaliações
- Jurnal Anak Ririn PDFDocumento10 páginasJurnal Anak Ririn PDFDexter BluesAinda não há avaliações
- Nejmoa1606356 PDFDocumento10 páginasNejmoa1606356 PDFDexter BluesAinda não há avaliações
- Fix ObgynDocumento17 páginasFix ObgynDexter BluesAinda não há avaliações
- PRM2016 1658172 PDFDocumento7 páginasPRM2016 1658172 PDFDexter BluesAinda não há avaliações
- Jurnal Anak RirinDocumento10 páginasJurnal Anak RirinDexter BluesAinda não há avaliações
- The Seven Cardinal MovementsDocumento4 páginasThe Seven Cardinal MovementsDexter BluesAinda não há avaliações
- Childhood IQ and Bipolar Link PDFDocumento9 páginasChildhood IQ and Bipolar Link PDFDexter BluesAinda não há avaliações
- Mood Dynamics in Bipolar Disorder: Research Open AccessDocumento9 páginasMood Dynamics in Bipolar Disorder: Research Open AccesswulanfarichahAinda não há avaliações
- Referat Obgyn FixDocumento29 páginasReferat Obgyn FixDexter BluesAinda não há avaliações
- 1830 PDF PDFDocumento5 páginas1830 PDF PDFDexter BluesAinda não há avaliações
- Childhood IQ and Bipolar Link PDFDocumento9 páginasChildhood IQ and Bipolar Link PDFDexter BluesAinda não há avaliações
- The Seven Cardinal MovementsDocumento4 páginasThe Seven Cardinal MovementsDexter BluesAinda não há avaliações
- Rincian Jadwal Jaga Koas Obsgin 2016 Senin Selas A Rabu Kami S Jumat Sabtu Mingg UDocumento1 páginaRincian Jadwal Jaga Koas Obsgin 2016 Senin Selas A Rabu Kami S Jumat Sabtu Mingg UDexter BluesAinda não há avaliações
- The Seven Cardinal MovementsDocumento3 páginasThe Seven Cardinal MovementsMaria Mandid0% (1)
- Pruritus: An Updated Look at An Old ProblemDocumento7 páginasPruritus: An Updated Look at An Old ProblemThariq Mubaraq DrcAinda não há avaliações
- Unchallengeable Miracles of QuranDocumento430 páginasUnchallengeable Miracles of QuranyoursincerefriendAinda não há avaliações
- Clinical Guidelines Acute Rehab Management 2010 InteractiveDocumento172 páginasClinical Guidelines Acute Rehab Management 2010 InteractivenathanaelandryAinda não há avaliações
- Jurnal Elderly 2 PDFDocumento3 páginasJurnal Elderly 2 PDFDexter BluesAinda não há avaliações
- TSWJ2015 803752 PDFDocumento8 páginasTSWJ2015 803752 PDFDexter BluesAinda não há avaliações
- Geriatric Itch PDFDocumento16 páginasGeriatric Itch PDFDexter BluesAinda não há avaliações
- GTA 05-08-018 Dust Supression AlternativesDocumento2 páginasGTA 05-08-018 Dust Supression Alternativesrickoshea160Ainda não há avaliações
- CGMP Learning Activity SheetDocumento4 páginasCGMP Learning Activity SheetJonille EchevarriaAinda não há avaliações
- Ocular InsertsDocumento15 páginasOcular InsertsPpa Gpat AmitAinda não há avaliações
- Minutes of 290th Meeting of Registration BoardDocumento1.286 páginasMinutes of 290th Meeting of Registration BoardUsman DarAinda não há avaliações
- Lichen PlanusDocumento6 páginasLichen PlanusMerry MiraAinda não há avaliações
- Ophthalmic Drug Delivery SystemsDocumento749 páginasOphthalmic Drug Delivery Systemskulbhushan singh100% (2)
- M.Pharm. (Pharmaceutical Analysis) : I Semester Theory Hours/weekDocumento11 páginasM.Pharm. (Pharmaceutical Analysis) : I Semester Theory Hours/weekgeorge robertAinda não há avaliações
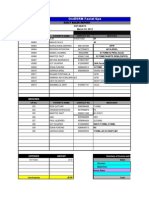
- OroDERM Facial Spa Daily Sales ReportDocumento12 páginasOroDERM Facial Spa Daily Sales ReportMarc Eric RedondoAinda não há avaliações
- Study Title Cytotoxicity Study Test On Extracts: SponsorDocumento28 páginasStudy Title Cytotoxicity Study Test On Extracts: SponsorCarlos Canedo HAinda não há avaliações
- Pharmaceutics 2 MCQ PDF DownloadDocumento7 páginasPharmaceutics 2 MCQ PDF DownloadDev Tyagi50% (2)
- A Systematic Review of Contact Dermatitis Treatment and PreventionDocumento24 páginasA Systematic Review of Contact Dermatitis Treatment and PreventionMuhammad Riza FahlawiAinda não há avaliações
- Loksewa AyogDocumento14 páginasLoksewa Ayogministore kmcAinda não há avaliações
- Fresh Bar Skincare and Haircare Product InventoryDocumento25 páginasFresh Bar Skincare and Haircare Product InventoryeraldaAinda não há avaliações
- BITTER GOURD Research ProposalDocumento3 páginasBITTER GOURD Research ProposalVerlynneAinda não há avaliações
- General Pharmacology 2013Documento403 páginasGeneral Pharmacology 2013tareAinda não há avaliações
- Routes of Administration ReferencesDocumento55 páginasRoutes of Administration ReferencesVictoria Eliza InguilloAinda não há avaliações
- Management of Cutaneous ErythrasmaDocumento11 páginasManagement of Cutaneous ErythrasmaDesi RatnaningtyasAinda não há avaliações
- How to prepare Burrow's solution for skin irritation reliefDocumento1 páginaHow to prepare Burrow's solution for skin irritation reliefJoanna Carla Marmonejo Estorninos-Walker100% (1)
- Daivonex Ointment, Cream and Scalp Solution: Consumer Medicine InformationDocumento8 páginasDaivonex Ointment, Cream and Scalp Solution: Consumer Medicine InformationatcAinda não há avaliações
- Dermatology Compounding IdeasDocumento3 páginasDermatology Compounding IdeasBillQueAinda não há avaliações
- Types of DFDocumento48 páginasTypes of DFIdenyi Daniel EwaAinda não há avaliações
- Finnaled Panchamrit With Pages RemovedDocumento16 páginasFinnaled Panchamrit With Pages RemovedSammy BhaiAinda não há avaliações
- Drug PreparationDocumento6 páginasDrug PreparationHaizel BieberAinda não há avaliações
- Phardose PreparationsDocumento8 páginasPhardose PreparationsJaica Mangurali TumulakAinda não há avaliações
- Product Overviewcoeic90001016 PDFDocumento4 páginasProduct Overviewcoeic90001016 PDFAFRIANSYAHAinda não há avaliações
- A. I Only: Philippine Association of Colleges of Pharmacy Pharmaceutical Dosage Forms QuestionDocumento43 páginasA. I Only: Philippine Association of Colleges of Pharmacy Pharmaceutical Dosage Forms QuestionClarenceAinda não há avaliações
- Panchkarma - Leech TherapyDocumento19 páginasPanchkarma - Leech Therapyriya100% (1)