Você também pode gostar
- Hiv Confiebre Amilsa Lipasa Levada y Anromalidades HematolgoicasDocumento4 páginasHiv Confiebre Amilsa Lipasa Levada y Anromalidades HematolgoicasAndresPimentelAlvarezAinda não há avaliações
- Indice Shock Delta 2016 Literatura Latinoamericana 2016 PDFDocumento5 páginasIndice Shock Delta 2016 Literatura Latinoamericana 2016 PDFAndresPimentelAlvarezAinda não há avaliações
- Guias DX Cushing Endocrine SocietyDocumento15 páginasGuias DX Cushing Endocrine SocietyAndresPimentelAlvarezAinda não há avaliações
- Nacos Mayuo Clinic ProceedingsDocumento17 páginasNacos Mayuo Clinic ProceedingsAndresPimentelAlvarezAinda não há avaliações
- AHA Infective Endo PDFDocumento55 páginasAHA Infective Endo PDFRoselily AmitaAinda não há avaliações
- MT2014-11-036-CLARKE Iron Deficiency Anemia PDFDocumento6 páginasMT2014-11-036-CLARKE Iron Deficiency Anemia PDFAndresPimentelAlvarezAinda não há avaliações
- Approach To ThrombocytopeniaDocumento8 páginasApproach To ThrombocytopeniaChairul Nurdin AzaliAinda não há avaliações
- CD14 Como Señal de Disminucion Dolor Postqx PDFDocumento3 páginasCD14 Como Señal de Disminucion Dolor Postqx PDFAndresPimentelAlvarezAinda não há avaliações
- Distributive Shock Clinical Presentation - History, Physical ExaminationDocumento5 páginasDistributive Shock Clinical Presentation - History, Physical ExaminationAndresPimentelAlvarezAinda não há avaliações
- Pubscatalog de LA Aabb 2018Documento27 páginasPubscatalog de LA Aabb 2018AndresPimentelAlvarezAinda não há avaliações
- War-Up Angina Exercies Europ J Cardio 2014 PDFDocumento6 páginasWar-Up Angina Exercies Europ J Cardio 2014 PDFAndresPimentelAlvarezAinda não há avaliações
- Cap 27 Guyton Preguntas PDFDocumento5 páginasCap 27 Guyton Preguntas PDFAndresPimentelAlvarezAinda não há avaliações
- Pubscatalog de LA Aabb 2018Documento27 páginasPubscatalog de LA Aabb 2018AndresPimentelAlvarezAinda não há avaliações
- Mexico Mexico City GuideDocumento85 páginasMexico Mexico City GuideAndresPimentelAlvarezAinda não há avaliações
- Effect of Surgical Treatmen On Voice Quality in Reinke Edema J Med Updates 2013Documento6 páginasEffect of Surgical Treatmen On Voice Quality in Reinke Edema J Med Updates 2013AndresPimentelAlvarezAinda não há avaliações
- Brjexppathol00255 0037 PDFDocumento13 páginasBrjexppathol00255 0037 PDFAndresPimentelAlvarezAinda não há avaliações
- Genetics of Colorectal Cancer (PDQ®) - Health Professional Version - National Cancer InstituteDocumento121 páginasGenetics of Colorectal Cancer (PDQ®) - Health Professional Version - National Cancer InstituteAndresPimentelAlvarezAinda não há avaliações
- Artikel - Filippini Anestesia para Pacinete Scon Drogas IlicitasDocumento10 páginasArtikel - Filippini Anestesia para Pacinete Scon Drogas IlicitasAndresPimentelAlvarezAinda não há avaliações
- Artikel - Filippini Anestesia para Pacinete Scon Drogas IlicitasDocumento10 páginasArtikel - Filippini Anestesia para Pacinete Scon Drogas IlicitasAndresPimentelAlvarezAinda não há avaliações
- Desflurane Versus Sevoflurane For Maintenance Of.17Documento7 páginasDesflurane Versus Sevoflurane For Maintenance Of.17AndresPimentelAlvarezAinda não há avaliações
- War-Up Angina Exercies Europ J Cardio 2014Documento6 páginasWar-Up Angina Exercies Europ J Cardio 2014AndresPimentelAlvarezAinda não há avaliações
- Understanding the Mechanisms of Acute Traumatic CoagulopathyDocumento32 páginasUnderstanding the Mechanisms of Acute Traumatic CoagulopathyAndresPimentelAlvarezAinda não há avaliações
- Cd14 Como Señal de Disminucion Dolor PostqxDocumento3 páginasCd14 Como Señal de Disminucion Dolor PostqxAndresPimentelAlvarezAinda não há avaliações
- Status Epileopticus Refractary Tto Con Isoflurano e Hipotermia Por 24 DiasDocumento6 páginasStatus Epileopticus Refractary Tto Con Isoflurano e Hipotermia Por 24 DiasAndresPimentelAlvarezAinda não há avaliações
- Venous Thrombosis in CirrhosisDocumento17 páginasVenous Thrombosis in CirrhosisAndresPimentelAlvarezAinda não há avaliações
- Venous Thrombosis in CirrhosisDocumento17 páginasVenous Thrombosis in CirrhosisAndresPimentelAlvarezAinda não há avaliações
- Aprv in Ards PDFDocumento10 páginasAprv in Ards PDFAndresPimentelAlvarezAinda não há avaliações
- Extubation Failure in Brain-Injured Patients Anesthesiology January 2017Documento11 páginasExtubation Failure in Brain-Injured Patients Anesthesiology January 2017AndresPimentelAlvarezAinda não há avaliações
- War-Up Angina Exercies Europ J Cardio 2014Documento6 páginasWar-Up Angina Exercies Europ J Cardio 2014AndresPimentelAlvarezAinda não há avaliações
- Levetiracetam EpilepsiaDocumento6 páginasLevetiracetam EpilepsiaAndresPimentelAlvarezAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Zwac189 PDFDocumento10 páginasZwac189 PDFWilliamAinda não há avaliações
- NUR3111 Past Paper Care PlanDocumento14 páginasNUR3111 Past Paper Care PlanliAinda não há avaliações
- Clinical Epidemiological and Evalutionary Profile of Strokes in Intensive Care of Neurology Fann Hospital in DakarDocumento5 páginasClinical Epidemiological and Evalutionary Profile of Strokes in Intensive Care of Neurology Fann Hospital in DakarCelebre MualabaAinda não há avaliações
- Recent Trends in The Pharmacotherapy of Angina Pectoris: ArticleDocumento14 páginasRecent Trends in The Pharmacotherapy of Angina Pectoris: ArticleLarysuka DenysukaAinda não há avaliações
- Sepsis-Induced Cardiomyopathy: A Comprehensive Review: Published Online: 6 May 2020Documento12 páginasSepsis-Induced Cardiomyopathy: A Comprehensive Review: Published Online: 6 May 2020Alicia GarcíaAinda não há avaliações
- Heart Anatomy and Function QuizDocumento8 páginasHeart Anatomy and Function QuizCharlz ZipaganAinda não há avaliações
- Elarde, Sylvia Somodio 2440010207Documento3 páginasElarde, Sylvia Somodio 2440010207Jenn ElardeAinda não há avaliações
- CRM Tendril Sts Pacing Lead CatalogDocumento2 páginasCRM Tendril Sts Pacing Lead CatalogsleonAinda não há avaliações
- MTE DR Mefri Cardiac ExaminationDocumento36 páginasMTE DR Mefri Cardiac ExaminationMuhammad Thariq Isnaini100% (1)
- G12 SUB 3rd Term 2022 Part 3 P.E Class Test QPDocumento9 páginasG12 SUB 3rd Term 2022 Part 3 P.E Class Test QPDourgesh RamlochunAinda não há avaliações
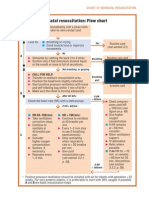
- Neonatal Resuscitation Program Flow ChartDocumento3 páginasNeonatal Resuscitation Program Flow ChartChin Nam80% (5)
- Incomplete Right Bundle-Branch Block: An Electrocardiographic MisnomerDocumento10 páginasIncomplete Right Bundle-Branch Block: An Electrocardiographic MisnomerxtineAinda não há avaliações
- Thrombosis Prevention by SlidesgoDocumento67 páginasThrombosis Prevention by SlidesgoRohanAinda não há avaliações
- Case Presentation of Hemorrhagic Stroke (Subarachnoid Hemorrhage)Documento69 páginasCase Presentation of Hemorrhagic Stroke (Subarachnoid Hemorrhage)verna88% (24)
- Thesis Statement For Cardiovascular DiseaseDocumento8 páginasThesis Statement For Cardiovascular DiseaseWebsiteThatWritesPapersForYouCanada100% (2)
- Group B Hypovolemic ShockDocumento22 páginasGroup B Hypovolemic ShockPam RomeroAinda não há avaliações
- InggrisDocumento13 páginasInggrisDefita DefitaAinda não há avaliações
- Obat Anti HipertensiDocumento9 páginasObat Anti Hipertensisilvanus giovannyAinda não há avaliações
- Guide Wire SelectionDocumento39 páginasGuide Wire SelectionPaula GuisardAinda não há avaliações
- Physiological indicators in exercise and fitnessDocumento11 páginasPhysiological indicators in exercise and fitnessElyon Shinohara50% (2)
- Acsm (042 082)Documento41 páginasAcsm (042 082)김동현Ainda não há avaliações
- Congestive Heart FailureDocumento43 páginasCongestive Heart Failure568563100% (1)
- Snow Shoveling SafetyDocumento2 páginasSnow Shoveling SafetyMichael JohnsonAinda não há avaliações
- Emergency Department Chest Pain Evaluation PathwayDocumento2 páginasEmergency Department Chest Pain Evaluation Pathwaymuhammad sajidAinda não há avaliações
- ECG Apib PDFDocumento68 páginasECG Apib PDFArthur KakarekoAinda não há avaliações
- Medicine IM Platinum-1Documento357 páginasMedicine IM Platinum-1Bom Tna67% (3)
- HypertensionSeoul2020 AbstractDocumento164 páginasHypertensionSeoul2020 AbstractRimaAinda não há avaliações
- Esc Congress 2016 ProgrammeDocumento2 páginasEsc Congress 2016 Programmejenitha jeniAinda não há avaliações
- Job DescriptionDocumento5 páginasJob DescriptionHarshavardhan SAinda não há avaliações
- ECG Criterias For Ventricular Hypertrophy by DR PRASANTH SDocumento13 páginasECG Criterias For Ventricular Hypertrophy by DR PRASANTH SnadineAinda não há avaliações