Você também pode gostar
- O&G Presentation GuidelineDocumento2 páginasO&G Presentation Guidelineleo90_wyattAinda não há avaliações
- Presentation Script ObsDocumento1 páginaPresentation Script ObsCk KmaAinda não há avaliações
- O&G Clerking ScriptDocumento4 páginasO&G Clerking ScriptA VHRSEAinda não há avaliações
- Obstetrics Case History by S.P.kamthankarDocumento7 páginasObstetrics Case History by S.P.kamthankarMd Ali0% (1)
- Case ReportDocumento19 páginasCase ReportvivitaslimAinda não há avaliações
- HX and PX Obstetrics and GynecologyDocumento21 páginasHX and PX Obstetrics and GynecologyTadesse MuhammedAinda não há avaliações
- History & Physical Exam in Ob/Gyn: By: - DR AmanuDocumento75 páginasHistory & Physical Exam in Ob/Gyn: By: - DR AmanuKåbåñå TürüñåAinda não há avaliações
- Neonatal History and Physical ExamDocumento2 páginasNeonatal History and Physical ExamMuhammad Farhan KhaliqAinda não há avaliações
- O and G Notes Notebank NumberedDocumento173 páginasO and G Notes Notebank NumberedPerscitus Ali القحطانيAinda não há avaliações
- OBGYN History and Exam EssentialsDocumento61 páginasOBGYN History and Exam EssentialsEthiopia TekdemAinda não há avaliações
- Reviewer For Pedia Osce: 10.5 KG 45.16 CM / 17.8 in 75 CM SixDocumento10 páginasReviewer For Pedia Osce: 10.5 KG 45.16 CM / 17.8 in 75 CM SixJamora ManilynAinda não há avaliações
- MBBS Course Regulations 231029 003955Documento31 páginasMBBS Course Regulations 231029 003955mkpaulAinda não há avaliações
- CASE 2 PneumoniaDocumento12 páginasCASE 2 PneumoniaKenneth MiguelAinda não há avaliações
- OBSTETRIC FORMDocumento4 páginasOBSTETRIC FORMKhylamarie VillalunaAinda não há avaliações
- New Intern Guide Quick NotesDocumento8 páginasNew Intern Guide Quick NotesTrisAinda não há avaliações
- Physio Ob ReviewDocumento368 páginasPhysio Ob ReviewMark LopezAinda não há avaliações
- Obstetrics History Taking in and Examination PowerpointDocumento15 páginasObstetrics History Taking in and Examination Powerpointياسر كوثر هانيAinda não há avaliações
- Gynaecology History Taking GuideDocumento7 páginasGynaecology History Taking GuideJahangir AlamAinda não há avaliações
- Neonatal Jaundice CaseDocumento6 páginasNeonatal Jaundice CaseRabi SyedAinda não há avaliações
- Gyne Case COCDocumento37 páginasGyne Case COCLian BaylosisAinda não há avaliações
- Disorders of Sex Development (DSD) DevelopmentDocumento40 páginasDisorders of Sex Development (DSD) DevelopmentAndi AdityaAinda não há avaliações
- OSCE Gynae HXDocumento3 páginasOSCE Gynae HXmpage3100% (1)
- Polyhydramnios and Oligohydramnios Clinical ExamDocumento2 páginasPolyhydramnios and Oligohydramnios Clinical ExamAhmad FahroziAinda não há avaliações
- Case Write Up FibroidDocumento17 páginasCase Write Up FibroidNadsri AmirAinda não há avaliações
- History and Pe ObgynDocumento4 páginasHistory and Pe ObgynCara Marrero IguidAinda não há avaliações
- History Taking OBS GYNDocumento10 páginasHistory Taking OBS GYNzvkznhsw2tAinda não há avaliações
- Pediatrics 2 LaboratoryDocumento40 páginasPediatrics 2 LaboratoryAmaetenAinda não há avaliações
- OB History Endorsement FormatDocumento6 páginasOB History Endorsement FormatVin CustodioAinda não há avaliações
- Systemic Surgery NuggetsDocumento17 páginasSystemic Surgery NuggetsAhmad UsmanAinda não há avaliações
- Osce ObgynDocumento37 páginasOsce ObgynDevi Christina Damanik (Papua medical School)Ainda não há avaliações
- Post Term PregnancyDocumento14 páginasPost Term PregnancySanthosh.S.UAinda não há avaliações
- Peads NotesDocumento130 páginasPeads NotesMadiha Shaikh100% (1)
- Sample SheetDocumento3 páginasSample SheetHamdy GabalAinda não há avaliações
- Serdang Protocol ObgynDocumento152 páginasSerdang Protocol ObgynNadhirah ZulkifliAinda não há avaliações
- Breast Abcess PDFDocumento4 páginasBreast Abcess PDFponekAinda não há avaliações
- HIV SeminarDocumento5 páginasHIV SeminarJoseph Velarde100% (2)
- Physical ExaminationgiDocumento61 páginasPhysical ExaminationgiHei LeeAinda não há avaliações
- Gynecology: Recurrent Pregnancy LossDocumento6 páginasGynecology: Recurrent Pregnancy LossDawn Marco100% (1)
- A Case of C.SDocumento85 páginasA Case of C.Sนีล ไบรอันAinda não há avaliações
- Kawasaki Disease DiagnosisDocumento5 páginasKawasaki Disease DiagnosisFranz SalazarAinda não há avaliações
- (IM Ward) History Taking Tool PDFDocumento15 páginas(IM Ward) History Taking Tool PDFleapacis100% (1)
- Breast Lump History: Opening The ConsultationDocumento2 páginasBreast Lump History: Opening The ConsultationYoyoguyAinda não há avaliações
- Fetal risks of macrosomia in diabetic pregnanciesDocumento27 páginasFetal risks of macrosomia in diabetic pregnanciesIful SaifullahAinda não há avaliações
- Paediatrics Case Report FINALDocumento14 páginasPaediatrics Case Report FINALMall Singh BhullarAinda não há avaliações
- Newborn NotesDocumento44 páginasNewborn NotesHaziq KamardinAinda não há avaliações
- OSCE Gynae-OSCE-MMSSDocumento24 páginasOSCE Gynae-OSCE-MMSSMohammad Saifullah100% (1)
- Gynecology 1.1 - History-Taking, Physical Examination, and Office GynecologyDocumento9 páginasGynecology 1.1 - History-Taking, Physical Examination, and Office GynecologyZaza100% (2)
- History Taking in ObgynDocumento17 páginasHistory Taking in Obgynselvie87100% (1)
- Endocrine Long CaseDocumento8 páginasEndocrine Long CaseNadia SalwaniAinda não há avaliações
- Clinical Case of Ulcer SurgeryDocumento5 páginasClinical Case of Ulcer SurgeryRachitha GuttaAinda não há avaliações
- Case Report Ca Cervix PDFDocumento44 páginasCase Report Ca Cervix PDFBianca PinkyAinda não há avaliações
- Approach To Patient With Ovarian Cysts: Done By: Yahyia Al-Abri 90440Documento53 páginasApproach To Patient With Ovarian Cysts: Done By: Yahyia Al-Abri 90440NinaAinda não há avaliações
- ICU Case: Septic Shock from Hospital-Acquired PneumoniaDocumento13 páginasICU Case: Septic Shock from Hospital-Acquired PneumoniaHana FauziAinda não há avaliações
- Obstetrics Case PresentationDocumento27 páginasObstetrics Case PresentationMahaprasad sahoo 77Ainda não há avaliações
- OSCE Reviewer 2013Documento4 páginasOSCE Reviewer 2013rere choiAinda não há avaliações
- Revision Long Case Obs GynaeDocumento10 páginasRevision Long Case Obs GynaeHo Yong WaiAinda não há avaliações
- History and Examination in Surgery GuideDocumento22 páginasHistory and Examination in Surgery Guidestephen X-SILVERAinda não há avaliações
- Contraction Stress Test complicationsDocumento5 páginasContraction Stress Test complicationsPao Ali100% (1)
- Taking Obstetrical HistoryDocumento20 páginasTaking Obstetrical Historymawada abdallaAinda não há avaliações
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- Mundane AstrologyDocumento93 páginasMundane Astrologynikhil mehra100% (5)
- 2020 Book WorkshopOnFrontiersInHighEnerg PDFDocumento456 páginas2020 Book WorkshopOnFrontiersInHighEnerg PDFSouravDeyAinda não há avaliações
- RumpelstiltskinDocumento7 páginasRumpelstiltskinAndreia PintoAinda não há avaliações
- Step-By-Step Guide To Essay WritingDocumento14 páginasStep-By-Step Guide To Essay WritingKelpie Alejandria De OzAinda não há avaliações
- Irony in Language and ThoughtDocumento2 páginasIrony in Language and Thoughtsilviapoli2Ainda não há avaliações
- Tong RBD3 SheetDocumento4 páginasTong RBD3 SheetAshish GiriAinda não há avaliações
- Skin Yale University Protein: Where Does Collagen Come From?Documento2 páginasSkin Yale University Protein: Where Does Collagen Come From?Ellaine Pearl AlmillaAinda não há avaliações
- 1 - Nature and Dev - Intl LawDocumento20 páginas1 - Nature and Dev - Intl Lawaditya singhAinda não há avaliações
- PIA Project Final PDFDocumento45 páginasPIA Project Final PDFFahim UddinAinda não há avaliações
- Food Product Development - SurveyDocumento4 páginasFood Product Development - SurveyJoan Soliven33% (3)
- Classification of Boreal Forest Ecosystem Goods and Services in FinlandDocumento197 páginasClassification of Boreal Forest Ecosystem Goods and Services in FinlandSivamani SelvarajuAinda não há avaliações
- SLE Case Report on 15-Year-Old GirlDocumento38 páginasSLE Case Report on 15-Year-Old GirlDiLa NandaRiAinda não há avaliações
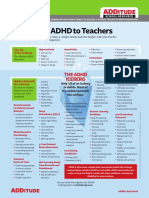
- Explaining ADHD To TeachersDocumento1 páginaExplaining ADHD To TeachersChris100% (2)
- Edition 100Documento30 páginasEdition 100Tockington Manor SchoolAinda não há avaliações
- MatriarchyDocumento11 páginasMatriarchyKristopher Trey100% (1)
- (Template) Grade 6 Science InvestigationDocumento6 páginas(Template) Grade 6 Science InvestigationYounis AhmedAinda não há avaliações
- Oyo Rooms-Case StudyDocumento13 páginasOyo Rooms-Case StudySHAMIK SHETTY50% (4)
- Economic Impact of Tourism in Greater Palm Springs 2023 CLIENT FINALDocumento15 páginasEconomic Impact of Tourism in Greater Palm Springs 2023 CLIENT FINALJEAN MICHEL ALONZEAUAinda não há avaliações
- Opportunity, Not Threat: Crypto AssetsDocumento9 páginasOpportunity, Not Threat: Crypto AssetsTrophy NcAinda não há avaliações
- Faxphone l100 Faxl170 l150 I-Sensys Faxl170 l150 Canofax L250seriesDocumento46 páginasFaxphone l100 Faxl170 l150 I-Sensys Faxl170 l150 Canofax L250seriesIon JardelAinda não há avaliações
- An Analysis of Students Pronounciation Errors Made by Ninth Grade of Junior High School 1 TengaranDocumento22 páginasAn Analysis of Students Pronounciation Errors Made by Ninth Grade of Junior High School 1 TengaranOcta WibawaAinda não há avaliações
- ACS Tech Manual Rev9 Vol1-TACTICS PDFDocumento186 páginasACS Tech Manual Rev9 Vol1-TACTICS PDFMihaela PecaAinda não há avaliações
- Topic 4: Mental AccountingDocumento13 páginasTopic 4: Mental AccountingHimanshi AryaAinda não há avaliações
- MW Scenario Handbook V 12 ADocumento121 páginasMW Scenario Handbook V 12 AWilliam HamiltonAinda não há avaliações
- Year 11 Economics Introduction NotesDocumento9 páginasYear 11 Economics Introduction Notesanon_3154664060% (1)
- IJAKADI: A Stage Play About Spiritual WarfareDocumento9 páginasIJAKADI: A Stage Play About Spiritual Warfareobiji marvelous ChibuzoAinda não há avaliações
- Neligence: Allows Standards of Acceptable Behavior To Be Set For SocietyDocumento3 páginasNeligence: Allows Standards of Acceptable Behavior To Be Set For SocietyransomAinda não há avaliações
- Tata Hexa (2017-2019) Mileage (14 KML) - Hexa (2017-2019) Diesel Mileage - CarWaleDocumento1 páginaTata Hexa (2017-2019) Mileage (14 KML) - Hexa (2017-2019) Diesel Mileage - CarWaleMahajan VickyAinda não há avaliações
- Jesus' Death on the Cross Explored Through Theological ModelsDocumento13 páginasJesus' Death on the Cross Explored Through Theological ModelsKhristian Joshua G. JuradoAinda não há avaliações
- Equity Inv HW 2 BHDocumento3 páginasEquity Inv HW 2 BHBen HolthusAinda não há avaliações