Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- NCLEX Drug CardsDocumento136 páginasNCLEX Drug CardsC Johnson100% (44)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- BloodDocumento51 páginasBloodDrShahid Sahito100% (1)
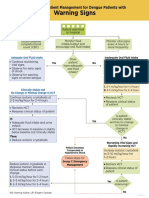
- B. Dengue Management Warning Signs InpatientDocumento1 páginaB. Dengue Management Warning Signs InpatientnrhmhealthAinda não há avaliações
- Yonex Badminton Catalog 2023 ENDocumento116 páginasYonex Badminton Catalog 2023 ENnrhmhealth100% (1)
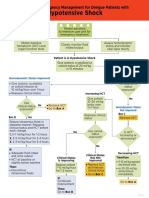
- C. Dengue Management HypotensiveShockDocumento1 páginaC. Dengue Management HypotensiveShocknrhmhealthAinda não há avaliações
- A. Management Dengue PatientsDocumento1 páginaA. Management Dengue PatientsnrhmhealthAinda não há avaliações
- D. Dengue Management CompensatedShockDocumento1 páginaD. Dengue Management CompensatedShocknrhmhealthAinda não há avaliações
- Dengue National Guidelines 2014Documento55 páginasDengue National Guidelines 2014nrhmhealthAinda não há avaliações
- Guidelines On Clinical Management of Covid - 19Documento15 páginasGuidelines On Clinical Management of Covid - 19shah007zaadAinda não há avaliações
- Noac GuidelinesDocumento40 páginasNoac GuidelinesCocosul Cocosului CocosaruluiAinda não há avaliações
- Revised 5x5 Matrix National Health MissionDocumento2 páginasRevised 5x5 Matrix National Health MissionnrhmhealthAinda não há avaliações
- Clinical Guidance On Diabetes Management at COVID-19 Patient Management FacilityDocumento14 páginasClinical Guidance On Diabetes Management at COVID-19 Patient Management FacilitynrhmhealthAinda não há avaliações
- Frequently Asked Questions On COVID-19 Vaccine: Target Group: General Public S. No. Potential ResponseDocumento8 páginasFrequently Asked Questions On COVID-19 Vaccine: Target Group: General Public S. No. Potential ResponseCNBCTV18 DigitalAinda não há avaliações
- Who Guidelines For Safe SurgeryDocumento173 páginasWho Guidelines For Safe SurgeryAhmed M Frieg100% (1)
- Standard For Female Male SterilizationDocumento104 páginasStandard For Female Male Sterilizationiman_kundu2007756Ainda não há avaliações
- Clinical Guidance On Diabetes Management at COVID-19 Patient Management FacilityDocumento14 páginasClinical Guidance On Diabetes Management at COVID-19 Patient Management FacilitynrhmhealthAinda não há avaliações
- RMNCH+A 5x5 MatrixDocumento1 páginaRMNCH+A 5x5 Matrixnrhmhealth100% (2)
- Standard Treatment Guidelines General Surgery: Ministry of Health & Family Welfare Govt. of IndiaDocumento73 páginasStandard Treatment Guidelines General Surgery: Ministry of Health & Family Welfare Govt. of IndiaiuytrerAinda não há avaliações
- Blunt Chest TraumaDocumento23 páginasBlunt Chest TraumanrhmhealthAinda não há avaliações
- 2015 Who Model List of Essential MedicinesDocumento53 páginas2015 Who Model List of Essential MedicinessallyAinda não há avaliações
- WHO - Clinical Guidelines PDFDocumento334 páginasWHO - Clinical Guidelines PDFnrhmhealthAinda não há avaliações
- WHO - Essential Drugs PDFDocumento376 páginasWHO - Essential Drugs PDFnrhmhealthAinda não há avaliações
- PCPNC BemoncDocumento180 páginasPCPNC BemoncBeryl de la CruzAinda não há avaliações
- Pocket Book of Hospital Care For ChildrenDocumento438 páginasPocket Book of Hospital Care For ChildrenTawangAinda não há avaliações
- PPIUCD Reference Manual-Feb 2011Documento81 páginasPPIUCD Reference Manual-Feb 2011nrhmhealthAinda não há avaliações
- STG - Obg PDFDocumento101 páginasSTG - Obg PDFnrhmhealthAinda não há avaliações
- District Planning Tool For Maternal and Newborn Health Strategy ImplementationDocumento67 páginasDistrict Planning Tool For Maternal and Newborn Health Strategy ImplementationnrhmhealthAinda não há avaliações
- Wound ManagementDocumento4 páginasWound ManagementnrhmhealthAinda não há avaliações
- Making Pregnancy Safer Safer Pregnancy in Tamil NaduDocumento100 páginasMaking Pregnancy Safer Safer Pregnancy in Tamil NaduUthayakumar KasthuriAinda não há avaliações
- Guia Reanimacion Neonatal OMSDocumento61 páginasGuia Reanimacion Neonatal OMSMarco RiveraAinda não há avaliações
- IMCI 2011 Chart BookletDocumento14 páginasIMCI 2011 Chart BookletYam Theresa Remo100% (1)
- Malaysia PharmaceuticalDocumento371 páginasMalaysia Pharmaceuticalching leeAinda não há avaliações
- Bell - S PalsyDocumento17 páginasBell - S PalsyRickzen Hawkins NikecholantAinda não há avaliações
- Public Health Microbiology - 3rd EdDocumento175 páginasPublic Health Microbiology - 3rd EdYolandia WAinda não há avaliações
- HAI BrochureDocumento6 páginasHAI BrochureNidia MaradiagaAinda não há avaliações
- 2016 December HixnewsDocumento50 páginas2016 December HixnewsAnonymous 4D6Dr5ScWAinda não há avaliações
- Case Study 4 RevisedDocumento9 páginasCase Study 4 RevisedHearts heavy Moms spaghettiAinda não há avaliações
- Basis DataDocumento2 páginasBasis DataAzzna AzAinda não há avaliações
- Pathology Lecture SeriesDocumento168 páginasPathology Lecture SeriesButch DumdumAinda não há avaliações
- History and Pathology of Vaccination by Edgar M. Crookshank, M.B. (1889)Documento560 páginasHistory and Pathology of Vaccination by Edgar M. Crookshank, M.B. (1889)puckett33100% (1)
- Pre-Operative Consent FormDocumento2 páginasPre-Operative Consent Formmsyafril1Ainda não há avaliações
- Role of Viral Infection in Sudden Hearing Loss: Xin Chen, Yao-Yao Fu and Tian-Yu ZhangDocumento8 páginasRole of Viral Infection in Sudden Hearing Loss: Xin Chen, Yao-Yao Fu and Tian-Yu Zhanggeraldi radityaAinda não há avaliações
- Ascaris LumbricoidesDocumento33 páginasAscaris LumbricoidesRosi Gustina100% (5)
- Cytogen ReviewerDocumento4 páginasCytogen ReviewerSophia Mae ClavecillaAinda não há avaliações
- (MT 6322 - MYCO VIRO LAB) Unit 8 Lab Diagnosis For Arboviruses, Roboviruses, dsRNADocumento3 páginas(MT 6322 - MYCO VIRO LAB) Unit 8 Lab Diagnosis For Arboviruses, Roboviruses, dsRNAAbbas MaghazehiAinda não há avaliações
- Management of Patient With AnemiaDocumento58 páginasManagement of Patient With AnemiaDoaa HussainAinda não há avaliações
- 1 s2.0 S0944501322000507 MainDocumento19 páginas1 s2.0 S0944501322000507 Mainsalmanurani warodatuszaqiahAinda não há avaliações
- Baveno VI Consensus Workshop 2015 PDFDocumento10 páginasBaveno VI Consensus Workshop 2015 PDFMadalina StoicescuAinda não há avaliações
- 100 Flash FinalDocumento107 páginas100 Flash FinalAshutosh FarkyaAinda não há avaliações
- Chapter 14 - StaphylococciDocumento36 páginasChapter 14 - StaphylococciVincent Reyes100% (1)
- BronchiolitisDocumento17 páginasBronchiolitisRizky DarmawanAinda não há avaliações
- Final Research Paper 1 Enc 1102 Tamryn Webb-GurleyDocumento11 páginasFinal Research Paper 1 Enc 1102 Tamryn Webb-Gurleyapi-490436143100% (1)
- Fixation of Mandibular Fractures With 2.0 MM MiniplatesDocumento7 páginasFixation of Mandibular Fractures With 2.0 MM MiniplatesRajan KarmakarAinda não há avaliações
- Biology Capsule For SSC CGL by StudyIQDocumento73 páginasBiology Capsule For SSC CGL by StudyIQstudyiq83% (6)
- OpisthorchisDocumento17 páginasOpisthorchisIqraAzizAinda não há avaliações
- NCP - Risk For InfectionDocumento3 páginasNCP - Risk For InfectionSiergs Smith Gervacio100% (3)
- Gram StainingDocumento9 páginasGram StainingGayatri PandaAinda não há avaliações
- ENT 2014 SovedDocumento7 páginasENT 2014 SovedHasnat HussainAinda não há avaliações
- Chapter 38: Human Diseases Caused by VirusesDocumento13 páginasChapter 38: Human Diseases Caused by Virusesharold_gravity9885Ainda não há avaliações