Você também pode gostar
- Ovarian 20 Cancer 1Documento39 páginasOvarian 20 Cancer 1Muhammad AL Farisi SutrisnoAinda não há avaliações
- Jurnal ObatDocumento17 páginasJurnal ObatMuhammad AL Farisi SutrisnoAinda não há avaliações
- OMSK B.ingDocumento4 páginasOMSK B.ingMuhammad AL Farisi SutrisnoAinda não há avaliações
- Tambahan 1Documento4 páginasTambahan 1Muhammad AL Farisi SutrisnoAinda não há avaliações
- Urticaria 2014Documento8 páginasUrticaria 2014Beny RaAinda não há avaliações
- HypovolaemicShock Alg PDFDocumento1 páginaHypovolaemicShock Alg PDFMuhammad AL Farisi SutrisnoAinda não há avaliações
- Journal Pone 0083261Documento11 páginasJournal Pone 0083261Muhammad AL Farisi SutrisnoAinda não há avaliações
- Urtikaria Kronik IdiopatikDocumento6 páginasUrtikaria Kronik IdiopatikgendisAinda não há avaliações
- A Critical Appraisal of Intravenous FluidsDocumento10 páginasA Critical Appraisal of Intravenous FluidsIrving H Torres LopezAinda não há avaliações
- Urogenital Imejing: DR - Ali Imran Lubis SP - RadDocumento16 páginasUrogenital Imejing: DR - Ali Imran Lubis SP - RadMuhammad AL Farisi SutrisnoAinda não há avaliações
- 4854Documento3 páginas4854Muhammad AL Farisi SutrisnoAinda não há avaliações
- Jurnal HypothyroidDocumento8 páginasJurnal HypothyroidMuhammad AL Farisi SutrisnoAinda não há avaliações
- C122Documento14 páginasC122anugerahAinda não há avaliações
- Crystalloid TeraphyDocumento9 páginasCrystalloid TeraphyMuhammad AL Farisi SutrisnoAinda não há avaliações
- Patofis SNDocumento12 páginasPatofis SNMuhammad AL Farisi SutrisnoAinda não há avaliações
- Nutritional Therapy in Pediatric Crohn Disease .22Documento5 páginasNutritional Therapy in Pediatric Crohn Disease .22mentariyuhendarAinda não há avaliações
- Management of Patients With Nephrotic Syndrome: Sophie de Seigneux, Pierre-Yves MartinDocumento7 páginasManagement of Patients With Nephrotic Syndrome: Sophie de Seigneux, Pierre-Yves MartinGarit Hapsari KiranaAinda não há avaliações
- C122Documento14 páginasC122anugerahAinda não há avaliações
- Pertanyaan2 SNDocumento8 páginasPertanyaan2 SNMuhammad AL Farisi SutrisnoAinda não há avaliações
- Nutrisi Dan TBCDocumento7 páginasNutrisi Dan TBCMuhammad AL Farisi SutrisnoAinda não há avaliações
- Jurnal Univ Sam RatulangiDocumento5 páginasJurnal Univ Sam RatulangiMink Ymk KazeAinda não há avaliações
- Quality Life After Tonsilectomy PDFDocumento8 páginasQuality Life After Tonsilectomy PDFMuhammad AL Farisi SutrisnoAinda não há avaliações
- Original Article: Evaluation of Microbial Flora in Chronic Tonsillitis and The Role of TonsillectomyDocumento5 páginasOriginal Article: Evaluation of Microbial Flora in Chronic Tonsillitis and The Role of TonsillectomyAmril BillahmarAinda não há avaliações
- Extraintestinal Manifestations in Children With.12Documento5 páginasExtraintestinal Manifestations in Children With.12Muhammad AL Farisi SutrisnoAinda não há avaliações
- Nutritional Therapy in Pediatric Crohn Disease .22Documento5 páginasNutritional Therapy in Pediatric Crohn Disease .22mentariyuhendarAinda não há avaliações
- Hydrolyzed Formulas For Allergy Prevention.7Documento4 páginasHydrolyzed Formulas For Allergy Prevention.7Muhammad AL Farisi SutrisnoAinda não há avaliações
- Use of Probiotics For Management of Acute.30Documento9 páginasUse of Probiotics For Management of Acute.30Muhammad AL Farisi SutrisnoAinda não há avaliações
- Tonsilitis Tahun 2011Documento3 páginasTonsilitis Tahun 2011Muhammad AL Farisi SutrisnoAinda não há avaliações
- Jurnal THTDocumento4 páginasJurnal THTNita RahmatunnisaAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Methods of ToiletDocumento180 páginasMethods of Toiletathegeha100% (2)
- Windy WigaDocumento2 páginasWindy WigaWindy wigaAinda não há avaliações
- 2015 Case 6 MBUDocumento12 páginas2015 Case 6 MBUDinesh TiwariAinda não há avaliações
- Anxiety Disorders BBDocumento18 páginasAnxiety Disorders BBRyan Justin BoudreauxAinda não há avaliações
- Subtotal Gastrectomy For Gastric CancerDocumento15 páginasSubtotal Gastrectomy For Gastric CancerRUBEN DARIO AGRESOTTAinda não há avaliações
- Chapter 1 Essay NegligenceDocumento3 páginasChapter 1 Essay NegligenceVladimir Hechavarria100% (1)
- The Letter of Intent To Enter PracticeDocumento4 páginasThe Letter of Intent To Enter Practicekazniels100% (1)
- Emqs ObsDocumento33 páginasEmqs Obsbakkiaha100% (1)
- AlprazolamDocumento10 páginasAlprazolamWen SilverAinda não há avaliações
- Crystal Aromatherapy Lesson 1Documento9 páginasCrystal Aromatherapy Lesson 1crystals21Ainda não há avaliações
- Hamstring Injuries in Football PDFDocumento276 páginasHamstring Injuries in Football PDFulfahrifAinda não há avaliações
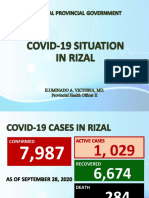
- Covid19 Situation in RizalDocumento23 páginasCovid19 Situation in RizalToni Quitalig GamezAinda não há avaliações
- Techniques For Parasite Egg Identification in Faecal SamplesDocumento9 páginasTechniques For Parasite Egg Identification in Faecal SamplesDr.Kedar Karki ,M.V.Sc.Preventive Vet.Medicine CLSU Philippines100% (2)
- 21 178 1 PBDocumento7 páginas21 178 1 PBClinica Dental AdvanceAinda não há avaliações
- Endocrine Glands The Producers of Chemical MessengersDocumento10 páginasEndocrine Glands The Producers of Chemical Messengersahmed100% (1)
- Abdominal BandagingDocumento34 páginasAbdominal BandagingStephanie Cyrelle Jane BacaniAinda não há avaliações
- Inguinal HerniaDocumento9 páginasInguinal HerniaAmanda RapaAinda não há avaliações
- HSE Campiagn - Safety Talk-01Documento2 páginasHSE Campiagn - Safety Talk-01NeeleshSoganiAinda não há avaliações
- Kampa VataDocumento27 páginasKampa VataAditya Tak100% (1)
- Flyer Camas Craniosacral TherapyDocumento3 páginasFlyer Camas Craniosacral TherapyAnonymous E7zHR3a5iAinda não há avaliações
- Medical Surgical Nursing ReviewDocumento97 páginasMedical Surgical Nursing ReviewBernadeth Josefa BorelaAinda não há avaliações
- Surgeon-Performed Ultrasound As A Diagnostic Tool in AppendicitisDocumento6 páginasSurgeon-Performed Ultrasound As A Diagnostic Tool in Appendicitisansar ahmedAinda não há avaliações
- Womens Era May (Second) 2010Documento148 páginasWomens Era May (Second) 2010ShaktirajanAinda não há avaliações
- Pha 613 Unit 1 Part 1 Terms - 10 StarDocumento56 páginasPha 613 Unit 1 Part 1 Terms - 10 StarBernadette ArnanteAinda não há avaliações
- NSCA Tools and Resources PDFDocumento3 páginasNSCA Tools and Resources PDFkunal mishraAinda não há avaliações
- Diana Sanchez V City & County of DenverDocumento48 páginasDiana Sanchez V City & County of DenverEllyn SantiagoAinda não há avaliações
- Diagnosis and Management of Subarachnoid HemorrhageDocumento25 páginasDiagnosis and Management of Subarachnoid HemorrhageMisael ClintonAinda não há avaliações
- IOL Masuk Keluar BM SDA NO Nama Obat Awal: Laporan BHP + Iol Ok Smec MojokertoDocumento6 páginasIOL Masuk Keluar BM SDA NO Nama Obat Awal: Laporan BHP + Iol Ok Smec MojokertoNaira Calya basagitaAinda não há avaliações
- Manual Neo 900Documento76 páginasManual Neo 900Bismarck Pablo Ibañez Piotti67% (3)
- Retinos PDFDocumento83 páginasRetinos PDFPaulo Gan100% (2)