Você também pode gostar
- Artículo Labriris (KMI-KMP)Documento7 páginasArtículo Labriris (KMI-KMP)Angela Maria SanchezAinda não há avaliações
- Assessing Progression of Keratoconus and Cross-Linking Efficacy The Belin ABCD Progression DisplayDocumento10 páginasAssessing Progression of Keratoconus and Cross-Linking Efficacy The Belin ABCD Progression DisplayJohn AlajoAinda não há avaliações
- Agreement of Kisa% and Kmax2 /TP in The Diagnosis of KeratoconusDocumento10 páginasAgreement of Kisa% and Kmax2 /TP in The Diagnosis of KeratoconusInternational Journal of Innovative Science and Research TechnologyAinda não há avaliações
- Comparison of Total Corneal Astigmatism Between IOLMasterDocumento7 páginasComparison of Total Corneal Astigmatism Between IOLMasterSarah Camacho PinedaAinda não há avaliações
- Keratoconus Corneal Posterior Surface Characterization According To The Degree of Visual LimitationDocumento7 páginasKeratoconus Corneal Posterior Surface Characterization According To The Degree of Visual LimitationGisela Palacios ArnedoAinda não há avaliações
- Corneal Asymmetry Analysis by Pentacam Scheimpflug Tomography For Keratoconus DiagnosisDocumento13 páginasCorneal Asymmetry Analysis by Pentacam Scheimpflug Tomography For Keratoconus DiagnosisJuanes MagnoAinda não há avaliações
- Comparative Corneal Topography and Refractive Variables in Monozygotic and Dizygotic TwinsDocumento6 páginasComparative Corneal Topography and Refractive Variables in Monozygotic and Dizygotic TwinsPotencia SalasAinda não há avaliações
- Beku 2Documento8 páginasBeku 2sri karuniaAinda não há avaliações
- 369 Full PDFDocumento8 páginas369 Full PDFTri Umi Maslakhatut DiniahAinda não há avaliações
- ARTICULO Evaluation of Corneal Shape and Biomechanics Before LASIK-minDocumento29 páginasARTICULO Evaluation of Corneal Shape and Biomechanics Before LASIK-minfiorellaAinda não há avaliações
- 1 s2.0 S0002939421006279 MainDocumento7 páginas1 s2.0 S0002939421006279 MainskocabzzAinda não há avaliações
- Assessment of Corneal Biomechanics, Tonometry and Pachymetry With The Corvis ST in MyopiaDocumento10 páginasAssessment of Corneal Biomechanics, Tonometry and Pachymetry With The Corvis ST in Myopiavergarajaviera548Ainda não há avaliações
- Development of Cephalometric Norms Using A UnifiedDocumento7 páginasDevelopment of Cephalometric Norms Using A UnifiedShannon Victor PeterAinda não há avaliações
- Score 1Documento18 páginasScore 1reva_90Ainda não há avaliações
- Trends in Corneal TopographyDocumento7 páginasTrends in Corneal TopographygustavoecardosoAinda não há avaliações
- 2010-02-17-1109CRSTEuro Ambrosio Rs Reprint PDFDocumento4 páginas2010-02-17-1109CRSTEuro Ambrosio Rs Reprint PDFYunisAinda não há avaliações
- Survey-62-P770 Keratoconus Review - QueratoconoDocumento14 páginasSurvey-62-P770 Keratoconus Review - QueratoconoMaría Antonela NicolóAinda não há avaliações
- 6401 FullDocumento7 páginas6401 FullYunita CahyadikaAinda não há avaliações
- Reduced Cross-Linking Demarcation Line Depth at The Peripheral Cornea After Corneal Collagen Cross-LinkingDocumento5 páginasReduced Cross-Linking Demarcation Line Depth at The Peripheral Cornea After Corneal Collagen Cross-LinkingMashhoor AlfayezAinda não há avaliações
- Comparison of Corneal Biomechanical Properties Among AxialDocumento8 páginasComparison of Corneal Biomechanical Properties Among AxialPutri kartiniAinda não há avaliações
- Refractive Error Changes in Cortical, Nuclear, and Posterior Subcapsular CataractsDocumento4 páginasRefractive Error Changes in Cortical, Nuclear, and Posterior Subcapsular CataractsAndi Ayu LestariAinda não há avaliações
- Novel Artificial Intelligence Index Based On.93Documento24 páginasNovel Artificial Intelligence Index Based On.93Alejandra VenegasAinda não há avaliações
- Lenstar IOLmasterDocumento6 páginasLenstar IOLmasterWillRoseroAinda não há avaliações
- Predicting Fuchs Endothelial Corneal Dystrophy Progression Using Scheimpflug TomographyDocumento9 páginasPredicting Fuchs Endothelial Corneal Dystrophy Progression Using Scheimpflug Tomographyinstagram googleAinda não há avaliações
- Long Term Follow-Up Safety and E Myopia Refractive Surgery: Ffectiveness ofDocumento9 páginasLong Term Follow-Up Safety and E Myopia Refractive Surgery: Ffectiveness ofayurAinda não há avaliações
- JCRSKCCustomized PARKcombined Topographic Refractivedatatreatmentof KeratoconusDocumento13 páginasJCRSKCCustomized PARKcombined Topographic Refractivedatatreatmentof KeratoconusDita Ambarsari SyafruddinAinda não há avaliações
- Central Corneal Thickness: Ultrasound Pachymetry Verus Anterior Segment Optical Coherence TomographyDocumento5 páginasCentral Corneal Thickness: Ultrasound Pachymetry Verus Anterior Segment Optical Coherence TomographybasharatAinda não há avaliações
- Clinical and Epidemiological Characterization of KeratoconusDocumento12 páginasClinical and Epidemiological Characterization of KeratoconusAndrés MontoyaAinda não há avaliações
- Catarat and MyopiaDocumento4 páginasCatarat and MyopiacsalvigAinda não há avaliações
- Feng Et Al 2023 Epithelial Thickness Mapping in Keratoconic Corneas Repeatability and Agreement Between Cso Ms 39Documento14 páginasFeng Et Al 2023 Epithelial Thickness Mapping in Keratoconic Corneas Repeatability and Agreement Between Cso Ms 39vahidsmpAinda não há avaliações
- Validation of An Objective Keratoconus Detection System Implemented in A Scheimpflug Tomographer and Comparison With Other MethodsDocumento7 páginasValidation of An Objective Keratoconus Detection System Implemented in A Scheimpflug Tomographer and Comparison With Other Methodstai daisyAinda não há avaliações
- Comparative Analysis of Refractive and Topographic Changes in Early and Advanced Keratoconic Eyes Undergoing Corneal Collagen CrosslinkingDocumento6 páginasComparative Analysis of Refractive and Topographic Changes in Early and Advanced Keratoconic Eyes Undergoing Corneal Collagen CrosslinkingMohamad Hasnol HayatAinda não há avaliações
- ABCD Progression Display For Keratoconus ProgressionDocumento5 páginasABCD Progression Display For Keratoconus ProgressionRamesh BabuAinda não há avaliações
- Catarct SinilisDocumento5 páginasCatarct SinilisAsri Mukti NantaAinda não há avaliações
- Ocular Aberrations Before and After Myopic Corneal Refractive Surgery: LASIK-Induced Changes Measured With Laser Ray TracingDocumento8 páginasOcular Aberrations Before and After Myopic Corneal Refractive Surgery: LASIK-Induced Changes Measured With Laser Ray Tracingbonny_07_fk_unsri9248Ainda não há avaliações
- Spectral Domain Optical Coherence Tomography Findings in - 2019 - Journal of CurDocumento6 páginasSpectral Domain Optical Coherence Tomography Findings in - 2019 - Journal of CurMichael John AguilarAinda não há avaliações
- Low Reliability of CBCT for Diagnosing TMJ Soft Tissue CalcificationDocumento5 páginasLow Reliability of CBCT for Diagnosing TMJ Soft Tissue CalcificationMarinaAinda não há avaliações
- Comparison Between Femtosecond Laser Mushroom Con Figuration and Manual Trephine Straight-Edge Con Figuration Deep Anterior Lamellar KeratoplastyDocumento6 páginasComparison Between Femtosecond Laser Mushroom Con Figuration and Manual Trephine Straight-Edge Con Figuration Deep Anterior Lamellar KeratoplastyindahdeshakaAinda não há avaliações
- PIIS000293942200407XDocumento13 páginasPIIS000293942200407XAnca Florina GaceaAinda não há avaliações
- Do Racial Differences in Orbital Volume Influence The Reconstruction of Orbital TraumaDocumento6 páginasDo Racial Differences in Orbital Volume Influence The Reconstruction of Orbital Traumashehla khanAinda não há avaliações
- Wang 2003Documento15 páginasWang 2003Milzan MurtadhaAinda não há avaliações
- In Vitro: Differential Diagnosis of Clavus and Verruca by A Predictive Model Generated From Electrical ImpedanceDocumento7 páginasIn Vitro: Differential Diagnosis of Clavus and Verruca by A Predictive Model Generated From Electrical ImpedanceGita ListawatiAinda não há avaliações
- Conductive Keratoplasty Corrects HyperopiaDocumento10 páginasConductive Keratoplasty Corrects HyperopiaAchmad Deddy FatoniAinda não há avaliações
- Clinical Study: Comparison of The Optical Quality Between Small Incision Lenticule Extraction and Femtosecond Laser LASIKDocumento10 páginasClinical Study: Comparison of The Optical Quality Between Small Incision Lenticule Extraction and Femtosecond Laser LASIKnicoAinda não há avaliações
- Accuracy of Two Devices and Three Different Calculation Methods For Predicting Residual Astigmatism After Intraocular Lens ImplantationDocumento5 páginasAccuracy of Two Devices and Three Different Calculation Methods For Predicting Residual Astigmatism After Intraocular Lens Implantationjorefe12Ainda não há avaliações
- البحث الخامسDocumento5 páginasالبحث الخامسReham Fawzy ElshinawyAinda não há avaliações
- Topographic Scoring System Identifies Glaucoma in Myopic EyesDocumento10 páginasTopographic Scoring System Identifies Glaucoma in Myopic EyesValentina Gracia ReyAinda não há avaliações
- Corneal Parameters Measurement in Healthy Subjects Using Scheimpflug and Anterior Segment Optical Coherence TomographyDocumento6 páginasCorneal Parameters Measurement in Healthy Subjects Using Scheimpflug and Anterior Segment Optical Coherence TomographyvahidsmpAinda não há avaliações
- Multi Class ClassificationDocumento20 páginasMulti Class ClassificationKrutika SapkalAinda não há avaliações
- Clinical Importance of The Lens Opacities Classification System III (LOCS III) in PhacoemulsificationDocumento4 páginasClinical Importance of The Lens Opacities Classification System III (LOCS III) in Phacoemulsificationnaveeduddin2001Ainda não há avaliações
- Inflammation and The Nervous System: The Connection in The Cornea in Patients With Infectious KeratitisDocumento8 páginasInflammation and The Nervous System: The Connection in The Cornea in Patients With Infectious KeratitisrizkydimasaputraAinda não há avaliações
- Keratoconus Screening Using Values Derived From Auto-Keratometer Measurements: A Multicenter StudyDocumento8 páginasKeratoconus Screening Using Values Derived From Auto-Keratometer Measurements: A Multicenter Study小島隆司Ainda não há avaliações
- Kjo 32 172Documento10 páginasKjo 32 172Nurul Dwi LestariAinda não há avaliações
- Accuracy of Clin. Tests 2020Documento12 páginasAccuracy of Clin. Tests 2020Ahmed MortadaAinda não há avaliações
- Contribution of Nuclear Morphometric Features To Differentiation of Atypical Complex Type Endometrial Hyperplasia and Low Grade Endometrial CarcinomaDocumento4 páginasContribution of Nuclear Morphometric Features To Differentiation of Atypical Complex Type Endometrial Hyperplasia and Low Grade Endometrial CarcinomaFerdina NidyasariAinda não há avaliações
- Methods For Assessing Corneal Opacity: Seminars in OphthalmologyDocumento7 páginasMethods For Assessing Corneal Opacity: Seminars in OphthalmologyGermán PérezAinda não há avaliações
- Ho 2010Documento6 páginasHo 2010Sarah Camacho PinedaAinda não há avaliações
- Ocular Biometry Among Cataract Surgery Candidate Patients in Southwestern EthiopiaDocumento17 páginasOcular Biometry Among Cataract Surgery Candidate Patients in Southwestern EthiopiaArdhienk LaodeAinda não há avaliações
- Controversies in the Management of KeratoconusNo EverandControversies in the Management of KeratoconusAdel BarbaraAinda não há avaliações
- Case Studies in Advanced Skin Cancer Management: An Osce Viva ResourceNo EverandCase Studies in Advanced Skin Cancer Management: An Osce Viva ResourceAinda não há avaliações
- CataractDocumento3 páginasCataractSetiawan Arif WibowoAinda não há avaliações
- Paediatrics and Child Health Volume 22 Issue 1 2012 (Doi 10.1016 - J.paed.2011.04.002) Patrick Watts - Preseptal and Orbital Cellulitis in Children - A ReviewDocumento8 páginasPaediatrics and Child Health Volume 22 Issue 1 2012 (Doi 10.1016 - J.paed.2011.04.002) Patrick Watts - Preseptal and Orbital Cellulitis in Children - A ReviewSetiawan Arif WibowoAinda não há avaliações
- Early Vs Late Traumatic CataractDocumento6 páginasEarly Vs Late Traumatic CataractSetiawan Arif WibowoAinda não há avaliações
- Papillitis DeleonjodyDocumento2 páginasPapillitis DeleonjodySetiawan Arif WibowoAinda não há avaliações
- Cotton Combed Round Neck 20's (Satuan) Ukuran Putih Hitam Warna LainDocumento2 páginasCotton Combed Round Neck 20's (Satuan) Ukuran Putih Hitam Warna LainSetiawan Arif WibowoAinda não há avaliações
- Selulitis PDFDocumento5 páginasSelulitis PDFDhisa Zainita HabsariAinda não há avaliações
- Amsler Grid PDFDocumento1 páginaAmsler Grid PDFSetiawan Arif WibowoAinda não há avaliações
- NIH Public Access: The Pathophysiology of Thyroid Eye Disease (TED) : Implications For ImmunotherapyDocumento10 páginasNIH Public Access: The Pathophysiology of Thyroid Eye Disease (TED) : Implications For ImmunotherapySetiawan Arif WibowoAinda não há avaliações
- CanaliculitisDocumento12 páginasCanaliculitisSetiawan Arif WibowoAinda não há avaliações
- Mayoclinic Management SEDocumento11 páginasMayoclinic Management SESetiawan Arif WibowoAinda não há avaliações
- 1 s2.0 S0146000515001962Documento14 páginas1 s2.0 S0146000515001962Setiawan Arif WibowoAinda não há avaliações
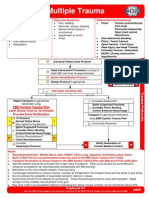
- Multiple Trauma ManagementDocumento1 páginaMultiple Trauma ManagementSetiawan Arif WibowoAinda não há avaliações
- Critical Appraisal of The International Subarachnoid Aneurysm Trial (ISAT)Documento7 páginasCritical Appraisal of The International Subarachnoid Aneurysm Trial (ISAT)Setiawan Arif WibowoAinda não há avaliações
- APH at Term: ABCs, Etiology, Diagnosis, ManagementDocumento26 páginasAPH at Term: ABCs, Etiology, Diagnosis, ManagementSetiawan Arif WibowoAinda não há avaliações
- Multiple Trauma EvaluationDocumento2 páginasMultiple Trauma EvaluationSetiawan Arif WibowoAinda não há avaliações
- Publications Safe AbortionDocumento110 páginasPublications Safe AbortionSetiawan Arif WibowoAinda não há avaliações
- Group 1 RDL2Documento101 páginasGroup 1 RDL2ChristelAinda não há avaliações
- Khin Thandar Myint EMPADocumento101 páginasKhin Thandar Myint EMPAAshin NandavamsaAinda não há avaliações
- Diversity and InclusionDocumento23 páginasDiversity and InclusionJasper Andrew Adjarani80% (5)
- Eng Listening Integrated Hkdse2022 UmayDocumento21 páginasEng Listening Integrated Hkdse2022 UmayHoi TungAinda não há avaliações
- Introduction To Tensors: Contravariant and Covariant VectorsDocumento18 páginasIntroduction To Tensors: Contravariant and Covariant VectorslilaAinda não há avaliações
- 1402 2046Documento11 páginas1402 2046Luca PilottiAinda não há avaliações
- Experiment 5 ADHAVANDocumento29 páginasExperiment 5 ADHAVANManoj Raj RajAinda não há avaliações
- Analyzing Evidence of College Readiness: A Tri-Level Empirical & Conceptual FrameworkDocumento66 páginasAnalyzing Evidence of College Readiness: A Tri-Level Empirical & Conceptual FrameworkJinky RegonayAinda não há avaliações
- Sakolsky Ron Seizing AirwavesDocumento219 páginasSakolsky Ron Seizing AirwavesPalin WonAinda não há avaliações
- Listening LP1Documento6 páginasListening LP1Zee KimAinda não há avaliações
- Evidence Law PDFDocumento15 páginasEvidence Law PDFwanborAinda não há avaliações
- Jobgpt 9d48h0joDocumento6 páginasJobgpt 9d48h0jomaijel CancinesAinda não há avaliações
- mc1776 - Datasheet PDFDocumento12 páginasmc1776 - Datasheet PDFLg GnilAinda não há avaliações
- Integrating GrammarDocumento8 páginasIntegrating GrammarMaría Perez CastañoAinda não há avaliações
- Engineering: Ronnapee Chaichaowarat, Jun Kinugawa, Kazuhiro KosugeDocumento8 páginasEngineering: Ronnapee Chaichaowarat, Jun Kinugawa, Kazuhiro Kosugelaura bemudezAinda não há avaliações
- How To Create A MetacogDocumento6 páginasHow To Create A Metacogdocumentos lleserAinda não há avaliações
- North American Indians - A Very Short IntroductionDocumento147 páginasNorth American Indians - A Very Short IntroductionsiesmannAinda não há avaliações
- Planning Levels and Types for Organizational SuccessDocumento20 páginasPlanning Levels and Types for Organizational SuccessLala Ckee100% (1)
- 02 Cost of Capital QBDocumento26 páginas02 Cost of Capital QBAbhi JayakumarAinda não há avaliações
- Cambridge IGCSE™: Chinese As A Second Language 0523/03 May/June 2021Documento6 páginasCambridge IGCSE™: Chinese As A Second Language 0523/03 May/June 2021For GamingAinda não há avaliações
- SMAW Product DevelopmentDocumento9 páginasSMAW Product Developmenttibo bursioAinda não há avaliações
- Ductile Brittle TransitionDocumento7 páginasDuctile Brittle TransitionAndrea CalderaAinda não há avaliações
- Global Trustworthiness 2022 ReportDocumento32 páginasGlobal Trustworthiness 2022 ReportCaroline PimentelAinda não há avaliações
- UTS - Comparative Literature - Indah Savitri - S1 Sastra Inggris - 101201001Documento6 páginasUTS - Comparative Literature - Indah Savitri - S1 Sastra Inggris - 101201001indahcantik1904Ainda não há avaliações
- Photojournale - Connections Across A Human PlanetDocumento75 páginasPhotojournale - Connections Across A Human PlanetjohnhorniblowAinda não há avaliações
- Richard Herrmann-Fractional Calculus - An Introduction For Physicists-World Scientific (2011)Documento274 páginasRichard Herrmann-Fractional Calculus - An Introduction For Physicists-World Scientific (2011)Juan Manuel ContrerasAinda não há avaliações
- Araminta Spook My Haunted House ExtractDocumento14 páginasAraminta Spook My Haunted House Extractsenuthmi dihansaAinda não há avaliações
- Existentialism Is A HumanismDocumento4 páginasExistentialism Is A HumanismAlex MendezAinda não há avaliações
- Modbus Quick StartDocumento3 páginasModbus Quick StartNash JungAinda não há avaliações
- Sample File: Official Game AccessoryDocumento6 páginasSample File: Official Game AccessoryJose L GarcíaAinda não há avaliações