Você também pode gostar
- Evidence Based MedicineDocumento23 páginasEvidence Based MedicineTejus Murthy A G100% (2)
- SUDsDocumento28 páginasSUDsTejus Murthy A GAinda não há avaliações
- Antidepressants: HistoryDocumento8 páginasAntidepressants: HistoryTejus Murthy A GAinda não há avaliações
- Projective Personality TestsDocumento13 páginasProjective Personality TestsTejus Murthy A G100% (3)
- Projective Personality TestsDocumento13 páginasProjective Personality TestsTejus Murthy A G100% (3)
- Projective Personality TestsDocumento43 páginasProjective Personality TestsTejus Murthy A G100% (1)
- Projective Personality TestsDocumento43 páginasProjective Personality TestsTejus Murthy A G100% (1)
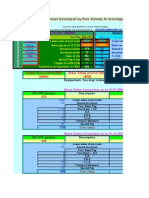
- 6th Central Pay Commission Salary CalculatorDocumento15 páginas6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Antipsychotics in ProdromeDocumento3 páginasAntipsychotics in ProdromeTejus Murthy A GAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (120)
- How Death Came To The CityDocumento3 páginasHow Death Came To The City789863Ainda não há avaliações
- 1.3 Digital Communication and AnalogueDocumento6 páginas1.3 Digital Communication and AnaloguenvjnjAinda não há avaliações
- Midterm Exam (Regulatory Framework and Legal Issues in Business Law) 2021 - Prof. Gerald SuarezDocumento4 páginasMidterm Exam (Regulatory Framework and Legal Issues in Business Law) 2021 - Prof. Gerald SuarezAlexandrea Bella Guillermo67% (3)
- Advisory Board ResearchDocumento6 páginasAdvisory Board Researcheaw12Ainda não há avaliações
- MIL Q3 Module 5 REVISEDDocumento23 páginasMIL Q3 Module 5 REVISEDEustass Kidd68% (19)
- BTCTL 17Documento5 páginasBTCTL 17Alvin BenaventeAinda não há avaliações
- Unit 6 Listening Practice OUT AND ABOUT 1Documento1 páginaUnit 6 Listening Practice OUT AND ABOUT 1Marta Sampedro GonzalezAinda não há avaliações
- VW Golf 2 Sam Naprawiam PDFDocumento3 páginasVW Golf 2 Sam Naprawiam PDFScottAinda não há avaliações
- Kematian Di ICUDocumento24 páginasKematian Di ICURahmida RahmyAinda não há avaliações
- ElectionDocumento127 páginasElectionRaviKumar50% (2)
- 2013 03 01 Maurizio Di Noia PresentationDocumento80 páginas2013 03 01 Maurizio Di Noia PresentationRene KotzeAinda não há avaliações
- Statistics On Lgbtiq Inclusion in NorwayDocumento46 páginasStatistics On Lgbtiq Inclusion in NorwayНиколай ВавиличевAinda não há avaliações
- World War I Almanac Almanacs of American WarsDocumento561 páginasWorld War I Almanac Almanacs of American WarsMatheus Benedito100% (1)
- Hapter 2: Theoretical FrameworkDocumento18 páginasHapter 2: Theoretical FrameworkMohamed HamzaAinda não há avaliações
- แนวข้อสอบเข้าม.1 อังกฤษ ชุดที่1Documento8 páginasแนวข้อสอบเข้าม.1 อังกฤษ ชุดที่1ณิชคุณ สอนคุ้มAinda não há avaliações
- Developing Mental Health-Care Quality Indicators: Toward A Common FrameworkDocumento6 páginasDeveloping Mental Health-Care Quality Indicators: Toward A Common FrameworkCarl FisherAinda não há avaliações
- Sec 25 HmaDocumento3 páginasSec 25 HmaMukul BajajAinda não há avaliações
- Interpret Market Trends and Developments TASk 1Documento7 páginasInterpret Market Trends and Developments TASk 1Raí SilveiraAinda não há avaliações
- A Book of Beasts PDFDocumento32 páginasA Book of Beasts PDFbrad drac100% (2)
- A Guide To Conducting A Systematic Literature Review ofDocumento51 páginasA Guide To Conducting A Systematic Literature Review ofDarryl WallaceAinda não há avaliações
- Models of CommunicationDocumento20 páginasModels of CommunicationTrisha Ray60% (5)
- Course Content: SAP Fiori Implementation (SAPX03)Documento3 páginasCourse Content: SAP Fiori Implementation (SAPX03)Jathin Varma KanumuriAinda não há avaliações
- Bootstrap Aggregating Multivariate Adaptive Regression Spline For Observational Studies in Diabetes CasesDocumento8 páginasBootstrap Aggregating Multivariate Adaptive Regression Spline For Observational Studies in Diabetes CasesTika MijayantiAinda não há avaliações
- 07.03.09 Chest PhysiotherapyDocumento10 páginas07.03.09 Chest PhysiotherapyMuhammad Fuad MahfudAinda não há avaliações
- Ponty Maurice (1942,1968) Structure of BehaviorDocumento131 páginasPonty Maurice (1942,1968) Structure of BehaviorSnorkel7Ainda não há avaliações
- LESSON 6 Perfect TensesDocumento4 páginasLESSON 6 Perfect TensesAULINO JÚLIOAinda não há avaliações
- Rule Against Multiplicity and Child PornoDocumento3 páginasRule Against Multiplicity and Child PornoHouston Criminal Lawyer John T. FloydAinda não há avaliações
- An Aging Game Simulation Activity For Al PDFDocumento13 páginasAn Aging Game Simulation Activity For Al PDFramzan aliAinda não há avaliações
- Short Tutorial On Recurrence RelationsDocumento13 páginasShort Tutorial On Recurrence RelationsAbdulfattah HusseinAinda não há avaliações
- Potential Nursing Diagnosis Problem Fdar / NCP: Activity # 2Documento2 páginasPotential Nursing Diagnosis Problem Fdar / NCP: Activity # 2Karl KiwisAinda não há avaliações