Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- NATIONAL GUIDELINES ON QUALITY OBSTETRICS AND PERINATAL CARE Final Feb 2022 PDFDocumento700 páginasNATIONAL GUIDELINES ON QUALITY OBSTETRICS AND PERINATAL CARE Final Feb 2022 PDFvincent obunga50% (2)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Pangmalakasan NP1Documento134 páginasPangmalakasan NP1MikEeAyanEsterasAinda não há avaliações
- Nursing Care of Male and Female Clients With General and Specific Problems in SexualityDocumento22 páginasNursing Care of Male and Female Clients With General and Specific Problems in SexualityDecere PascualAinda não há avaliações
- l3 Immunization & Cold ChainDocumento53 páginasl3 Immunization & Cold ChainNur AinaaAinda não há avaliações
- Instruments & IndicationsDocumento11 páginasInstruments & IndicationsZiyad100% (2)
- Patient-Centered Communication: Exploring The Dentist's Role in The Era of E-Patients and Health 2.0Documento8 páginasPatient-Centered Communication: Exploring The Dentist's Role in The Era of E-Patients and Health 2.0shargunan11Ainda não há avaliações
- DR Ward ClassDocumento36 páginasDR Ward ClassChristy Mutia AlumbroAinda não há avaliações
- Akanksha Gupta FinalDraft - WHO - WordDocumento114 páginasAkanksha Gupta FinalDraft - WHO - WordAkanksha GuptaAinda não há avaliações
- Concepts of DiseaseDocumento54 páginasConcepts of DiseaseKailash NagarAinda não há avaliações
- Calcium HypochloriteDocumento7 páginasCalcium HypochloriteFrancois BresseAinda não há avaliações
- Hiv and AidsDocumento32 páginasHiv and AidsWelfredo Jr YuAinda não há avaliações
- Hygiene and Human HealthDocumento69 páginasHygiene and Human HealthRalu OroszAinda não há avaliações
- Toronto CA - Rest of The World Should Learn From Canada-Toronto CA (2023)Documento3 páginasToronto CA - Rest of The World Should Learn From Canada-Toronto CA (2023)haroldpsbAinda não há avaliações
- Soc 01 Project 2 NutritionDocumento13 páginasSoc 01 Project 2 Nutritionapi-354675795Ainda não há avaliações
- HANDWASHING NARRATIVEDocumento5 páginasHANDWASHING NARRATIVECaroline FernandezAinda não há avaliações
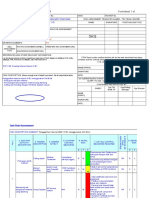
- Level 2 Risk Assessment for MMC VI-BX Internal ReplacementDocumento14 páginasLevel 2 Risk Assessment for MMC VI-BX Internal ReplacementAndi Yanuar50% (2)
- SCOSAN VI ProceedingsDocumento307 páginasSCOSAN VI ProceedingsrupakhasanAinda não há avaliações
- Case LawsDocumento205 páginasCase LawsSonu PandaAinda não há avaliações
- Concept Map of Maternity CareDocumento3 páginasConcept Map of Maternity CareKristineAinda não há avaliações
- FMT Clinical Application FrameworkDocumento19 páginasFMT Clinical Application FrameworkElGatoDeAuronplay0% (1)
- Breastfeeding InfoDocumento2 páginasBreastfeeding InfoThe Vancouver SunAinda não há avaliações
- Wise consumer guidelines for health informationDocumento3 páginasWise consumer guidelines for health informationRainier DoctoleroAinda não há avaliações
- Irr Ra 11712Documento11 páginasIrr Ra 11712Learsi Afable100% (1)
- Final DraftDocumento5 páginasFinal Draftapi-451064930Ainda não há avaliações
- Hospital Acquired Infection (HAI) Prevention and Control MeasuresDocumento27 páginasHospital Acquired Infection (HAI) Prevention and Control MeasuresBharath G MahendrakarAinda não há avaliações
- Should Minors Be Able To Purchase Birth Control Without Parental ConsentDocumento4 páginasShould Minors Be Able To Purchase Birth Control Without Parental ConsentjohnAinda não há avaliações
- Perspectives in Public HealthDocumento50 páginasPerspectives in Public HealthDabala Harish ReddyAinda não há avaliações
- Part4 Evidence1 CozineDocumento2 páginasPart4 Evidence1 Cozineapi-286143658Ainda não há avaliações
- Project - Based - Learning: Exploration of Elements in NatureDocumento10 páginasProject - Based - Learning: Exploration of Elements in NatureAleeya MaisarahAinda não há avaliações
- (TCALLP) Right of ChildrenDocumento19 páginas(TCALLP) Right of ChildrenMaria CristinaAinda não há avaliações