Você também pode gostar
- ASH Hematology Review Series - AML - Sallman D - 6-2022Documento60 páginasASH Hematology Review Series - AML - Sallman D - 6-2022Иван НегарэAinda não há avaliações
- Cases Study in Plasma Cell DyscrasiaDocumento87 páginasCases Study in Plasma Cell Dyscrasiadrafq2000Ainda não há avaliações
- 3908 FullDocumento7 páginas3908 FullJavier MedinaAinda não há avaliações
- Non-Hodgkin Lymphoma and Hodgkin's Disease: From The Transplantation's Point of ViewDocumento46 páginasNon-Hodgkin Lymphoma and Hodgkin's Disease: From The Transplantation's Point of ViewFikri HariqiAinda não há avaliações
- Tavil 2016Documento3 páginasTavil 2016Alfredo Enrique Marin AliagaAinda não há avaliações
- Cardiac Toxicity Following High-Dose Cyclophosphamide, Cisplatin, and BCNU (STAMP-I) For Breast CancerDocumento6 páginasCardiac Toxicity Following High-Dose Cyclophosphamide, Cisplatin, and BCNU (STAMP-I) For Breast CancerNenad MladenovicAinda não há avaliações
- MDS MPN2019 DR Rachel SalitDocumento39 páginasMDS MPN2019 DR Rachel Salitluca.win92Ainda não há avaliações
- Prognostic Relevance of The Expression of TDT and CD7 in 335 Cases of Acute Myeloid LeukemiaDocumento8 páginasPrognostic Relevance of The Expression of TDT and CD7 in 335 Cases of Acute Myeloid LeukemiaAnonymous iqoU1mtAinda não há avaliações
- Survival PcaDocumento6 páginasSurvival PcaMuhammad Arie Wibisono RangkutiAinda não há avaliações
- Acute Leukemias: Case PresentationDocumento14 páginasAcute Leukemias: Case PresentationFrankenstein MelancholyAinda não há avaliações
- Xavier Leleu 2012Documento10 páginasXavier Leleu 2012monday125Ainda não há avaliações
- Myelodysplastic Syndromes1Documento26 páginasMyelodysplastic Syndromes1api-205355237Ainda não há avaliações
- International Phase 3 Study of Azacitidine Vs Conventional Care Regimens in Older Patients With Newly Diagnosed AML With 30% BlastsDocumento9 páginasInternational Phase 3 Study of Azacitidine Vs Conventional Care Regimens in Older Patients With Newly Diagnosed AML With 30% BlastsOrxan HumbetovAinda não há avaliações
- Trastuzumab en Adyuvancia: Mr2 Sally Paredes Noguni Hnerm - Oncologia MedicaDocumento20 páginasTrastuzumab en Adyuvancia: Mr2 Sally Paredes Noguni Hnerm - Oncologia MedicaSally Paredes NoguniAinda não há avaliações
- 1 - Hodgkin's LymphomaDocumento12 páginas1 - Hodgkin's LymphomaDiana MitreaAinda não há avaliações
- Acute Leukaemia Presentation 1Documento20 páginasAcute Leukaemia Presentation 1Vaibhav KrishnaAinda não há avaliações
- MTOR Inhibitor Nanoparticle Albumin-Bound (Nab (R) ) Rapamycin Is Effective in A Breast Cancer Xenograft ModelDocumento1 páginaMTOR Inhibitor Nanoparticle Albumin-Bound (Nab (R) ) Rapamycin Is Effective in A Breast Cancer Xenograft ModelTira MaharaniAinda não há avaliações
- New England Journal Medicine: The ofDocumento10 páginasNew England Journal Medicine: The ofanggiAinda não há avaliações
- Medicine2 - Myeloproliferative, Lymphoproliferative WorkshopDocumento118 páginasMedicine2 - Myeloproliferative, Lymphoproliferative Workshopapi-3762917100% (1)
- Cpho025 02 06Documento12 páginasCpho025 02 06Kyung-Nam KohAinda não há avaliações
- 2023 - Online Trial Questions (Academy 2020-2021-2022)Documento33 páginas2023 - Online Trial Questions (Academy 2020-2021-2022)Ruxandra BănicăAinda não há avaliações
- Apl 1Documento45 páginasApl 1api-243480627Ainda não há avaliações
- PSB MGCH - OdpDocumento22 páginasPSB MGCH - OdpdrpsbAinda não há avaliações
- 2010-09!16!161642 Allotransplant For RIchtersDocumento3 páginas2010-09!16!161642 Allotransplant For RIchtersdoctorniravAinda não há avaliações
- Paediatric AML Guidance Dec 2015Documento33 páginasPaediatric AML Guidance Dec 2015Genetic Clinic UKMAinda não há avaliações
- Glynne Jones2015Documento3 páginasGlynne Jones2015Robert ChristevenAinda não há avaliações
- Imaging in Peripheral Arterial Disease: Clinical and Research ApplicationsNo EverandImaging in Peripheral Arterial Disease: Clinical and Research ApplicationsAinda não há avaliações
- Barb Melo SkyDocumento17 páginasBarb Melo SkyAfiqah So JasmiAinda não há avaliações
- Chemoregimen - Testicular CancerDocumento2 páginasChemoregimen - Testicular CancerNanda Asyura RizkyaniAinda não há avaliações
- Acute Myeloid LeukemiaDocumento20 páginasAcute Myeloid LeukemiahemendreAinda não há avaliações
- MMDocumento67 páginasMMRatnaAinda não há avaliações
- ESMO Examination Answers To Trial QuestionsDocumento32 páginasESMO Examination Answers To Trial QuestionsVlad Croitoru100% (1)
- PBC 24420Documento7 páginasPBC 24420Nachapol JatAinda não há avaliações
- Karen A. Gelmon: Desmoplastic Small Round-Cell Tumor of The PancreasDocumento3 páginasKaren A. Gelmon: Desmoplastic Small Round-Cell Tumor of The PancreasAdam HartonoAinda não há avaliações
- Liver TransplantDocumento16 páginasLiver TransplantNephrology On-DemandAinda não há avaliações
- FDA Approval Summary - Atezolizumab and Durvalumab in Combination With Platinum-Based Chemotherapy in Extensive Stage Small Cell Lung CancerDocumento6 páginasFDA Approval Summary - Atezolizumab and Durvalumab in Combination With Platinum-Based Chemotherapy in Extensive Stage Small Cell Lung CancerasdffdsaAinda não há avaliações
- Project Presentation-Sydney StratfordDocumento17 páginasProject Presentation-Sydney Stratfordapi-611918048Ainda não há avaliações
- CCO Gastric Cancer LL SlidesDocumento63 páginasCCO Gastric Cancer LL SlidesPoncho Silva100% (1)
- Davis Symposium AdvancesInSarcomaDocumento55 páginasDavis Symposium AdvancesInSarcomaFernando SilalahiAinda não há avaliações
- Denosumab For Treatment of Hypercalcemia of MalignancyDocumento9 páginasDenosumab For Treatment of Hypercalcemia of MalignancySandra PargaAinda não há avaliações
- Plasma Cell NeoplasmsDocumento36 páginasPlasma Cell Neoplasmsdrafq2000Ainda não há avaliações
- Novel Diagnostic and Predictive Biomarkers in Pancreatic AdenocarcinomaDocumento14 páginasNovel Diagnostic and Predictive Biomarkers in Pancreatic AdenocarcinomaChavdarAinda não há avaliações
- If HP Cancer Guide BMT ManualDocumento363 páginasIf HP Cancer Guide BMT ManualZardar KAinda não há avaliações
- F-FDG Pet/Ct and I-Metaiodobenzylguanidine Imaging in High-Risk Neuroblastoma: Diagnostic Comparison and Survival AnalysisDocumento7 páginasF-FDG Pet/Ct and I-Metaiodobenzylguanidine Imaging in High-Risk Neuroblastoma: Diagnostic Comparison and Survival AnalysisManos PanagiotidisAinda não há avaliações
- Lang 2015Documento5 páginasLang 2015Diego SantoroAinda não há avaliações
- Biol Blood Marrow Transplant 21 (2015) 653e660Documento8 páginasBiol Blood Marrow Transplant 21 (2015) 653e660Rhinaldy DanaraAinda não há avaliações
- PembrolizumabDocumento25 páginasPembrolizumabFernando Emanuel Olmedo BroemserAinda não há avaliações
- Furtado 2016Documento10 páginasFurtado 2016zzzzAinda não há avaliações
- Reuter 2010Documento8 páginasReuter 2010Hector Javier BurgosAinda não há avaliações
- FluidDocumento190 páginasFluidAndrias OzAinda não há avaliações
- Acondicinamiento en LmaDocumento8 páginasAcondicinamiento en LmaRom ÁlvAinda não há avaliações
- Aproximación A La LLA T Del AdultoDocumento9 páginasAproximación A La LLA T Del AdultoJuan Antonio LópezAinda não há avaliações
- CML IM Drug-Free Ross Haematologica 2012Documento3 páginasCML IM Drug-Free Ross Haematologica 2012JuniaAinda não há avaliações
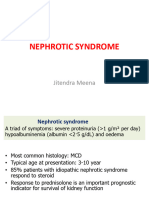
- SRNSDocumento19 páginasSRNSpedsoncoaiimsAinda não há avaliações
- Permenkes Tentang Penetapan Nilai KritisDocumento34 páginasPermenkes Tentang Penetapan Nilai KritisMeutia sariAinda não há avaliações
- AURORA: Is There A Role For Statin Therapy in Dialysis Patients?Documento4 páginasAURORA: Is There A Role For Statin Therapy in Dialysis Patients?Ravan WidiAinda não há avaliações
- Multiple MyelomaDocumento23 páginasMultiple Myelomabubbu92Ainda não há avaliações
- Fast Facts: Measurable Residual Disease: A clearer picture for treatment decisionsNo EverandFast Facts: Measurable Residual Disease: A clearer picture for treatment decisionsAinda não há avaliações
- Five Characteristics of Authentic LeadershipDocumento2 páginasFive Characteristics of Authentic LeadershipArnel Billy LimAinda não há avaliações
- Governance StructureDocumento1 páginaGovernance StructureJoydip MukhopadhyayAinda não há avaliações
- (ISPS Book Series) Yrjö O. Alanen, Manuel González de Chávez, Ann-Louise S. Silver, Brian Martindale - Psychotherapeutic Approaches To Schizophrenic Psychoses - Past, Present and Future-Routledge (20Documento419 páginas(ISPS Book Series) Yrjö O. Alanen, Manuel González de Chávez, Ann-Louise S. Silver, Brian Martindale - Psychotherapeutic Approaches To Schizophrenic Psychoses - Past, Present and Future-Routledge (20Manuel100% (1)
- LYON Conditions of Secondment 3500EUR enDocumento4 páginasLYON Conditions of Secondment 3500EUR enabdu1lahAinda não há avaliações
- Insulating Oil TestingDocumento6 páginasInsulating Oil TestingnasrunAinda não há avaliações
- An Assignment On "Mycology Laboratory Technique"Documento1 páginaAn Assignment On "Mycology Laboratory Technique"BsksvdndkskAinda não há avaliações
- Transmission Lines SMART EDGE VILLARUEL For April 2024 v1Documento89 páginasTransmission Lines SMART EDGE VILLARUEL For April 2024 v1mayandichoso24Ainda não há avaliações
- EHEDG Guidelines by Topics 04 2013Documento2 páginasEHEDG Guidelines by Topics 04 2013renzolonardi100% (1)
- Do Statins Lower TestosteroneDocumento3 páginasDo Statins Lower TestosteroneNandia SeptiyoriniAinda não há avaliações
- 224 Chinese Healing ExercisesDocumento4 páginas224 Chinese Healing ExercisesKiné Therapeut-manuelle Masseur GabiAinda não há avaliações
- The Way Out of Alcoholism by Jack BolandDocumento38 páginasThe Way Out of Alcoholism by Jack BolandIma AardvarkAinda não há avaliações
- PBL 2 Case PresentationDocumento12 páginasPBL 2 Case PresentationRamish IrfanAinda não há avaliações
- MCS120 220 Error Ref - GAA30082DAC - RefDocumento21 páginasMCS120 220 Error Ref - GAA30082DAC - RefCoil98Ainda não há avaliações
- 1 PolarographyDocumento20 páginas1 PolarographyRiya Das100% (1)
- Contemporary ImageDocumento43 páginasContemporary ImageProf. L100% (1)
- Ethics, Privacy, and Security: Lesson 14Documento16 páginasEthics, Privacy, and Security: Lesson 14Jennifer Ledesma-Pido100% (1)
- The Aging Brain: Course GuidebookDocumento126 páginasThe Aging Brain: Course GuidebookIsabel Cristina Jaramillo100% (2)
- EESC 111 Worksheets Module 5Documento5 páginasEESC 111 Worksheets Module 5Keira O'HowAinda não há avaliações
- LM 337Documento4 páginasLM 337matias robertAinda não há avaliações
- NCP Ineffective Breathing ActualDocumento3 páginasNCP Ineffective Breathing ActualArian May Marcos100% (1)
- ATR4518R6v07: Antenna SpecificationsDocumento2 páginasATR4518R6v07: Antenna Specificationsanna.bAinda não há avaliações
- KL 4 Unit 6 TestDocumento3 páginasKL 4 Unit 6 TestMaciej Koififg0% (1)
- Marketing ProjectDocumento82 páginasMarketing ProjectSumit GuptaAinda não há avaliações
- Women and International Human Rights Law PDFDocumento67 páginasWomen and International Human Rights Law PDFakilasriAinda não há avaliações
- Uppercut MagazineDocumento12 páginasUppercut MagazineChris Finn100% (1)
- Iso 15011-2-2009Documento26 páginasIso 15011-2-2009marcosAinda não há avaliações
- Immobilization of E. Coli Expressing Bacillus Pumilus CynD in Three Organic Polymer MatricesDocumento23 páginasImmobilization of E. Coli Expressing Bacillus Pumilus CynD in Three Organic Polymer MatricesLUIS CARLOS ROMERO ZAPATAAinda não há avaliações
- On How To Design A Low Voltage SwitchboardDocumento11 páginasOn How To Design A Low Voltage SwitchboardsabeerAinda não há avaliações
- Injection Analyzer Electronic Unit enDocumento67 páginasInjection Analyzer Electronic Unit enmayralizbethbustosAinda não há avaliações
- Dermatology Mini-OSCEDocumento322 páginasDermatology Mini-OSCEMarrkAinda não há avaliações