Você também pode gostar
- Acute Glomerulonep Hritis: By: Edelrose D. Lapitan BSN Iii-CDocumento29 páginasAcute Glomerulonep Hritis: By: Edelrose D. Lapitan BSN Iii-CEdelrose Lapitan100% (1)
- Hepatic Encephalopathy: Causes, Tests, and Treatment OptionsNo EverandHepatic Encephalopathy: Causes, Tests, and Treatment OptionsNota: 3.5 de 5 estrelas3.5/5 (2)
- AnemiaDocumento2 páginasAnemiaLazeh MeAinda não há avaliações
- Liver DiseasesDocumento29 páginasLiver DiseasesRicaneth TaanAinda não há avaliações
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- Renal DisordersDocumento77 páginasRenal Disorderslorelee_espaldon100% (1)
- Cystic FibrosisDocumento203 páginasCystic FibrosisAren SongcoAinda não há avaliações
- Anatomy of The KidneysDocumento7 páginasAnatomy of The KidneysSanthu SuAinda não há avaliações
- Urinary Tract CalculiDocumento34 páginasUrinary Tract CalculiOnkar SinghAinda não há avaliações
- Lecture Signs and Symptoms of Cardiovascular System DiseasesDocumento240 páginasLecture Signs and Symptoms of Cardiovascular System DiseasesMihaela IonescuAinda não há avaliações
- College of Nursing: Civil HospitalDocumento15 páginasCollege of Nursing: Civil HospitalDipal Jignesh PatelAinda não há avaliações
- Understanding Low Blood Pressure - The BasicsDocumento6 páginasUnderstanding Low Blood Pressure - The BasicsRajeev Nechiyil100% (1)
- Gastro Intestinal Bleeding DR - muayAD ABASSDocumento59 páginasGastro Intestinal Bleeding DR - muayAD ABASSMAFADHELAinda não há avaliações
- Acute Renal Failure: Dr. Bobi Ahmad S, S.KPDocumento62 páginasAcute Renal Failure: Dr. Bobi Ahmad S, S.KPdr.Bobi Ahmad Sahid, S.KepAinda não há avaliações
- Disseminated Intravascular Coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandDisseminated Intravascular Coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- Congenital Heart DiseasesDocumento21 páginasCongenital Heart DiseasesfahmiAinda não há avaliações
- Assessment of The Peripheral Vascular SystemDocumento17 páginasAssessment of The Peripheral Vascular SystemgrailbadAinda não há avaliações
- Ks Module 12Documento29 páginasKs Module 12jerinthomasrajanAinda não há avaliações
- Function of G I System: The Primary Digestive Functions Are Break Down Food Particles "Documento113 páginasFunction of G I System: The Primary Digestive Functions Are Break Down Food Particles "cherryann_12100% (1)
- I.V. FluidsDocumento33 páginasI.V. FluidsVineel Bezawada100% (1)
- Congestive Heart FailureDocumento43 páginasCongestive Heart Failure568563100% (1)
- Approach To HyponatremiaDocumento47 páginasApproach To HyponatremiaRajiv MedankiAinda não há avaliações
- Cardiac ComplicationDocumento12 páginasCardiac ComplicationResa ShotsAinda não há avaliações
- Hyper-coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandHyper-coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- Renal AbscessDocumento10 páginasRenal AbscessRaghu Rajan100% (1)
- Cad PamphletDocumento2 páginasCad Pamphletapi-546509005Ainda não há avaliações
- Distributive Shock 1Documento41 páginasDistributive Shock 1Fuzi HannyAinda não há avaliações
- Urinary Tract Infection: AM Nicholson MB BS DM (Med Micro)Documento55 páginasUrinary Tract Infection: AM Nicholson MB BS DM (Med Micro)Steven IStudy SmithAinda não há avaliações
- Chronic Kidney Disease OverviewDocumento15 páginasChronic Kidney Disease Overviewjames100% (1)
- SepsisDocumento33 páginasSepsisv_vijayakanth7656Ainda não há avaliações
- Atherosclerosis 2 2017 (Modified)Documento64 páginasAtherosclerosis 2 2017 (Modified)Remo B AbyAinda não há avaliações
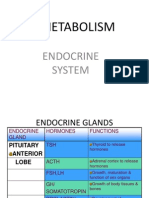
- Metabolism: Endocrine SystemDocumento129 páginasMetabolism: Endocrine SystemCodered Review100% (1)
- 01 - Signs and Symptoms of Git DisordersDocumento51 páginas01 - Signs and Symptoms of Git DisordersRere AnugrahAinda não há avaliações
- Heart Failure: Zelalem T., MD Yr III Resident, PediatricsDocumento65 páginasHeart Failure: Zelalem T., MD Yr III Resident, PediatricsChalie MequanentAinda não há avaliações
- Week 11 - Ch. 36 - UrinaryDocumento27 páginasWeek 11 - Ch. 36 - UrinaryMary SingletonAinda não há avaliações
- ShockDocumento21 páginasShockMin-Joo Esther ParkAinda não há avaliações
- Principles of Liver TransplantationDocumento22 páginasPrinciples of Liver TransplantationRajarshi KumarAinda não há avaliações
- Lab Values and Vital SignsDocumento4 páginasLab Values and Vital SignsWole Olaluwoye100% (1)
- Chirosis HepaticDocumento8 páginasChirosis HepaticCikalHrAinda não há avaliações
- Liver Cirrhosis: DR Alex MogereDocumento51 páginasLiver Cirrhosis: DR Alex MogereGladys Maina100% (1)
- Renal CalculiDocumento10 páginasRenal CalculiHarpreet Singh100% (1)
- The Breast: AnatomyDocumento3 páginasThe Breast: AnatomyRyan James Lorenzo Miguel50% (2)
- Intravenous Fluid Therapy in Adults in The HospitalDocumento28 páginasIntravenous Fluid Therapy in Adults in The Hospitalushapadminivadivelswamy100% (2)
- Newborn EmergenciesDocumento83 páginasNewborn EmergencieshwelpAinda não há avaliações
- Oncology Lectures 1 7 DR - FerrolinoDocumento24 páginasOncology Lectures 1 7 DR - FerrolinoMiguel Cuevas DolotAinda não há avaliações
- Ms. Meghana Goswami 1 Year M.SC M.B.N.CDocumento12 páginasMs. Meghana Goswami 1 Year M.SC M.B.N.CmeghanaAinda não há avaliações
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsNo EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsAinda não há avaliações
- Fluid and Electrolyte ImbalanceDocumento27 páginasFluid and Electrolyte ImbalanceSimmi Sidhu100% (1)
- Pregnancy Kidney DiseaseDocumento18 páginasPregnancy Kidney DiseaseMihai PavaleanAinda não há avaliações
- Renal StoneDocumento8 páginasRenal Stonevirz23Ainda não há avaliações
- Nephrotic Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandNephrotic Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- Drug StudyDocumento9 páginasDrug StudyJannefer HernandezAinda não há avaliações
- Congestive Heart FailureDocumento43 páginasCongestive Heart FailuresudersonAinda não há avaliações
- Urinary Retention 2Documento3 páginasUrinary Retention 2Agli AdhityaAinda não há avaliações
- Management of ShockDocumento12 páginasManagement of ShockMuhamad HilmiAinda não há avaliações
- Inguinal Hernias and Abdominal Wall Defects: Murad Nuserat & Abd AL-Rahman AlhelwDocumento51 páginasInguinal Hernias and Abdominal Wall Defects: Murad Nuserat & Abd AL-Rahman AlhelwRashed ShatnawiAinda não há avaliações
- Constipation 508Documento12 páginasConstipation 508Shishir Kumar SinghAinda não há avaliações
- Cough, Dyspnea and HemoptysisDocumento34 páginasCough, Dyspnea and HemoptysisPooja ShashidharanAinda não há avaliações
- Parkinson's DiseaseDocumento69 páginasParkinson's DiseaseSarfarazJerajAinda não há avaliações
- Erq419 05Documento7 páginasErq419 05Demuel Dee L. BertoAinda não há avaliações
- Anatomy QuizbeeDocumento39 páginasAnatomy QuizbeeDemuel Dee L. BertoAinda não há avaliações
- Molecular and Serological Investigation of 2019 nCoV Infected Patients Implication of Multiple Shedding RoutesDocumento5 páginasMolecular and Serological Investigation of 2019 nCoV Infected Patients Implication of Multiple Shedding RoutesDemuel Dee L. BertoAinda não há avaliações
- OSCE Checklist Cervical Screening SmearDocumento2 páginasOSCE Checklist Cervical Screening SmearDemuel Dee L. BertoAinda não há avaliações
- Erq120 07Documento7 páginasErq120 07Demuel Dee L. BertoAinda não há avaliações
- Anatomy QuizbeeDocumento39 páginasAnatomy QuizbeeDemuel Dee L. BertoAinda não há avaliações
- Erq419 10Documento7 páginasErq419 10Demuel Dee L. BertoAinda não há avaliações
- Badri2018 Article TheEffectsOfHomeAndSchoolOnChiDocumento16 páginasBadri2018 Article TheEffectsOfHomeAndSchoolOnChiDemuel Dee L. BertoAinda não há avaliações
- Endocrinology Board Review: Thyroid DisordersDocumento46 páginasEndocrinology Board Review: Thyroid DisordersDemuel Dee L. BertoAinda não há avaliações
- Association of Pseudo Meigs Syndrome With Struma Ovarii and High CA125 Mimicking Ovarian Malignancy GOROJ 2 113 PDFDocumento5 páginasAssociation of Pseudo Meigs Syndrome With Struma Ovarii and High CA125 Mimicking Ovarian Malignancy GOROJ 2 113 PDFDemuel Dee L. BertoAinda não há avaliações
- 1temperature RegulationDocumento51 páginas1temperature RegulationDemuel Dee L. BertoAinda não há avaliações
- Coronary CirculationDocumento47 páginasCoronary CirculationSuresh KumarAinda não há avaliações
- Happiness, Quality of Sleep and Academic Achievement Among University UndergraduatesDocumento1 páginaHappiness, Quality of Sleep and Academic Achievement Among University UndergraduatesDemuel Dee L. BertoAinda não há avaliações
- Primary Adrenal InsufficiencyDocumento28 páginasPrimary Adrenal InsufficiencyDemuel Dee L. BertoAinda não há avaliações
- Chapt4 EctodermDocumento16 páginasChapt4 EctodermDemuel Dee L. BertoAinda não há avaliações
- How To Develop A Super Memory and Learn Like A Genius With Jim Kwik Nov 2018 LaunchDocumento12 páginasHow To Develop A Super Memory and Learn Like A Genius With Jim Kwik Nov 2018 LaunchCarolina Ávila67% (3)
- Chronotype Differences in Timing of Energy and Macronutrient Intakes: A Population-Based Study in AdultsDocumento8 páginasChronotype Differences in Timing of Energy and Macronutrient Intakes: A Population-Based Study in AdultsDemuel Dee L. BertoAinda não há avaliações
- Temperature RegulationDocumento51 páginasTemperature RegulationDemuel Dee L. BertoAinda não há avaliações
- Cross Sectional Appraisal ToolDocumento4 páginasCross Sectional Appraisal ToolWuri Kusuma AtmajaAinda não há avaliações
- Development of The Musculoskeletal System: DR - Sahar HafeezDocumento24 páginasDevelopment of The Musculoskeletal System: DR - Sahar HafeezDemuel Dee L. BertoAinda não há avaliações
- Cell CommunicationDocumento55 páginasCell CommunicationDemuel Dee L. BertoAinda não há avaliações
- Exercise Physiology & Fitness: ©2009 Mcgraw-Hill Higher Education. All Rights ReservedDocumento51 páginasExercise Physiology & Fitness: ©2009 Mcgraw-Hill Higher Education. All Rights ReservedDemuel Dee L. BertoAinda não há avaliações
- Philippines Peoplve Living With HIV Stigma Index Report Cond FromOctober 2009 To January 2010Documento59 páginasPhilippines Peoplve Living With HIV Stigma Index Report Cond FromOctober 2009 To January 2010Demuel Dee L. BertoAinda não há avaliações
- Chapt4 EctodermDocumento16 páginasChapt4 EctodermDemuel Dee L. BertoAinda não há avaliações
- Anatomical ChartsDocumento2 páginasAnatomical ChartsDemuel Dee L. BertoAinda não há avaliações
- Philippines Peoplve Living With HIV Stigma Index Report Cond FromOctober 2009 To January 2010Documento59 páginasPhilippines Peoplve Living With HIV Stigma Index Report Cond FromOctober 2009 To January 2010Demuel Dee L. BertoAinda não há avaliações
- Anatomical ChartsDocumento2 páginasAnatomical ChartsDemuel Dee L. BertoAinda não há avaliações
- Awl 234Documento5 páginasAwl 234GiselleAinda não há avaliações
- Courage Under FireDocumento56 páginasCourage Under FireDemuel Dee L. BertoAinda não há avaliações
- Newborn Vital Signs ExaminationDocumento1 páginaNewborn Vital Signs ExaminationDemuel Dee L. BertoAinda não há avaliações
- The Prevalence and Associated Risk Factors of Musculoskeletal Disorders Among BankersDocumento21 páginasThe Prevalence and Associated Risk Factors of Musculoskeletal Disorders Among BankersNdayambaje EmmanuelAinda não há avaliações
- Neonatology Mock Exam 6 PDFDocumento6 páginasNeonatology Mock Exam 6 PDFMostafa Mahmoud Elsebey100% (2)
- Primery Survey GadarDocumento11 páginasPrimery Survey GadarapryAinda não há avaliações
- Psychopharmacology in Psychopharmacology in Psychiatry PsychiatryDocumento16 páginasPsychopharmacology in Psychopharmacology in Psychiatry PsychiatryHasnain HyderAinda não há avaliações
- Nursing Interview Guide To Collect Subjective Data From The Client Questions RationaleDocumento19 páginasNursing Interview Guide To Collect Subjective Data From The Client Questions RationaleKent Rebong100% (1)
- RMS Case Study (Leptospirosis) GRP 1 BSTM 1-B FinalDocumento12 páginasRMS Case Study (Leptospirosis) GRP 1 BSTM 1-B FinalLauren Abas Dela CruzAinda não há avaliações
- Use of Rare Remedies in Homoeopathic Practice: Dr. Ayush Kumar GuptaDocumento8 páginasUse of Rare Remedies in Homoeopathic Practice: Dr. Ayush Kumar GuptaIndhumathiAinda não há avaliações
- Executive Order No. 003-ADocumento2 páginasExecutive Order No. 003-AAndrew Murray D. DuranoAinda não há avaliações
- Residence Hall Application 2012Documento2 páginasResidence Hall Application 2012Theo ChandlerAinda não há avaliações
- Septic ShockDocumento11 páginasSeptic Shockj.doe.hex_87100% (1)
- PATHOPHYSIODocumento3 páginasPATHOPHYSIORomm JacobAinda não há avaliações
- Management of Asthma: A Guide To The Essentials of Good Clinical PracticeDocumento100 páginasManagement of Asthma: A Guide To The Essentials of Good Clinical Practicemalvika chawlaAinda não há avaliações
- ACDIS White Paper - How To Review A Medical RecordDocumento19 páginasACDIS White Paper - How To Review A Medical RecordCamille05100% (1)
- Herbal MedicinesDocumento8 páginasHerbal MedicinesKrishna BalsarzaAinda não há avaliações
- Dr. G. M. Taori: Curriculum VitaeDocumento12 páginasDr. G. M. Taori: Curriculum Vitaesrajan sahuAinda não há avaliações
- Personal Health Narrative 1Documento4 páginasPersonal Health Narrative 1api-592901792Ainda não há avaliações
- Vector Borne Disease Malaria Dengue Kalazar Chikungunya Filiarisis Indian Council Medical ResearchDocumento44 páginasVector Borne Disease Malaria Dengue Kalazar Chikungunya Filiarisis Indian Council Medical Researchanupsingh775Ainda não há avaliações
- OPD Rot Exam StudentDocumento3 páginasOPD Rot Exam StudentFerdinand TerceroAinda não há avaliações
- EntDocumento3 páginasEntmerna hazazahAinda não há avaliações
- The Grey Matter: Something in The AirDocumento28 páginasThe Grey Matter: Something in The AirMinaz PatelAinda não há avaliações
- Puskesmas Sako: Pemerintah Kota Palembang Dinas KesehatanDocumento7 páginasPuskesmas Sako: Pemerintah Kota Palembang Dinas KesehatandiniayuAinda não há avaliações
- Seizure-Case StudyDocumento6 páginasSeizure-Case StudyELaine ELena TiongsonAinda não há avaliações
- General AnesthesiaDocumento15 páginasGeneral AnesthesiaMahsaAinda não há avaliações
- History (Awasir)Documento37 páginasHistory (Awasir)Yousef TaqatqehAinda não há avaliações
- Respiratory Syncytial Virus in LowerDocumento6 páginasRespiratory Syncytial Virus in LowerShailendra ParajuliAinda não há avaliações
- Jurnal SleDocumento2 páginasJurnal SlePratidina Dwinda HEAinda não há avaliações
- Effects of High TSHDocumento3 páginasEffects of High TSHSreream KumarAinda não há avaliações
- Intro To EPDocumento48 páginasIntro To EPusfcards100% (2)
- Voluntary Self-Identification of Disability Form CC-305Documento1 páginaVoluntary Self-Identification of Disability Form CC-305kAinda não há avaliações
- Osteonecrosis: Avascular NecrosisDocumento8 páginasOsteonecrosis: Avascular NecrosisJezreel BonaAinda não há avaliações