Você também pode gostar
- Retinoblastoma - (Reh-Tin-Oh-BlastDocumento18 páginasRetinoblastoma - (Reh-Tin-Oh-BlastRoi GamasAinda não há avaliações
- Medical Case of Retinoblastoma in a 2-Year Old ChildDocumento14 páginasMedical Case of Retinoblastoma in a 2-Year Old ChildRafieLugassektiAinda não há avaliações
- Biology Investigatory Project: Samiksha Subhashish SarkarDocumento35 páginasBiology Investigatory Project: Samiksha Subhashish SarkarSamiksha SarkarAinda não há avaliações
- Retinoblastoma Case Report Latest With ReferenceDocumento29 páginasRetinoblastoma Case Report Latest With ReferenceMasykur Ramadhan GaniAinda não há avaliações
- Leukocoria. It Is Caused by Light Refl Ected Off The White Tumor Rather ThanDocumento4 páginasLeukocoria. It Is Caused by Light Refl Ected Off The White Tumor Rather ThanocisazakiahAinda não há avaliações
- Everything You Need to Know About Eye CancerDocumento15 páginasEverything You Need to Know About Eye CancerVince DinsayAinda não há avaliações
- Occupational Health Tips On Eye Protection For Good Visual HealthNo EverandOccupational Health Tips On Eye Protection For Good Visual HealthAinda não há avaliações
- About Retinoblastoma: Birmingham Children's HospitalDocumento3 páginasAbout Retinoblastoma: Birmingham Children's HospitalDwicky Limbersia AriesAinda não há avaliações
- Introduction To Eye Disorders-1Documento11 páginasIntroduction To Eye Disorders-1bhavani GAinda não há avaliações
- Macular Degeneration: From Diagnosis to TreatmentNo EverandMacular Degeneration: From Diagnosis to TreatmentNota: 4 de 5 estrelas4/5 (2)
- Low Vision: Assessment and Educational Needs: A Guide to Teachers and ParentsNo EverandLow Vision: Assessment and Educational Needs: A Guide to Teachers and ParentsAinda não há avaliações
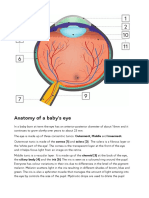
- Anatomy of A Baby's Eye: Outermost, Middle and Innermost. Cornea (1) and Sclera (2) - The Sclera Is A Fibrous Layer orDocumento2 páginasAnatomy of A Baby's Eye: Outermost, Middle and Innermost. Cornea (1) and Sclera (2) - The Sclera Is A Fibrous Layer orSandor GyongyverAinda não há avaliações
- Macular Degeneration: A Complete Guide for Patients and Their FamiliesNo EverandMacular Degeneration: A Complete Guide for Patients and Their FamiliesNota: 5 de 5 estrelas5/5 (1)
- Hey, Doc! What’S Wrong with My Eye?: A General Guide to Eye SymptomsNo EverandHey, Doc! What’S Wrong with My Eye?: A General Guide to Eye SymptomsAinda não há avaliações
- Retinal Detachment: Case Report Operating RoomDocumento30 páginasRetinal Detachment: Case Report Operating RoomCarlo Joseph Intal LlacerAinda não há avaliações
- Cranio Syn Ostos IsDocumento8 páginasCranio Syn Ostos IsDamal An NasherAinda não há avaliações
- Onisha Biology Project 14 10 15Documento14 páginasOnisha Biology Project 14 10 15Jelani GreerAinda não há avaliações
- Literature Review On Refractive ErrorsDocumento5 páginasLiterature Review On Refractive Errorsafmzfvlopbchbe100% (1)
- Retinoblastoma: What Is Cancer?Documento41 páginasRetinoblastoma: What Is Cancer?RizkyAgustriaAinda não há avaliações
- A Project On " Human Eye": Submitted To-Submitted byDocumento13 páginasA Project On " Human Eye": Submitted To-Submitted byaman1990100% (1)
- Reffractive ErrorsDocumento13 páginasReffractive ErrorsSagiraju SrinuAinda não há avaliações
- Eye Health / Blindness: Is An Eye Condition With Blurred Vision As Its Main Symptom. The Front Surface of TheDocumento10 páginasEye Health / Blindness: Is An Eye Condition With Blurred Vision As Its Main Symptom. The Front Surface of TheJulie BoAinda não há avaliações
- Research Paper On EyeosDocumento8 páginasResearch Paper On Eyeoskwbfbzund100% (1)
- Retinal Detachment: Case Report Operating RoomDocumento35 páginasRetinal Detachment: Case Report Operating RoomCarlo Joseph Intal Llacer50% (2)
- Biology Investigatory Project On Eye DiseasesDocumento18 páginasBiology Investigatory Project On Eye DiseasesBHALAJI KARUNANITHI100% (1)
- Biology Investigatory Project (On Eye Diseases)Documento22 páginasBiology Investigatory Project (On Eye Diseases)diya65% (49)
- Basic Eye ExamDocumento8 páginasBasic Eye ExamLisa AguilarAinda não há avaliações
- Literature Review Eye DiseasesDocumento7 páginasLiterature Review Eye Diseaseseqcusqwgf100% (1)
- Childhood Cataracts and Other JadiDocumento49 páginasChildhood Cataracts and Other JadiSania NadianisaAinda não há avaliações
- Eye Diseases: An Investigatory Project by Shrikanth Pillai XII BDocumento11 páginasEye Diseases: An Investigatory Project by Shrikanth Pillai XII BCR7STUDIO 7100% (1)
- LASIK: A Guide to Laser Vision CorrectionNo EverandLASIK: A Guide to Laser Vision CorrectionNota: 2.5 de 5 estrelas2.5/5 (2)
- Intracranial Tumors: An Ophthalmic Perspective: DR M Hemanandini, DR P Sumathi, DR P A KochamiDocumento3 páginasIntracranial Tumors: An Ophthalmic Perspective: DR M Hemanandini, DR P Sumathi, DR P A Kochamiwolfang2001Ainda não há avaliações
- Third Eye Research PaperDocumento7 páginasThird Eye Research Papertmiykcaod100% (1)
- Ebook 20Documento8 páginasEbook 20Eusivia PasiAinda não há avaliações
- Approach To Pediatric Periorbital EdemaDocumento10 páginasApproach To Pediatric Periorbital EdemaismailtaaaAinda não há avaliações
- Pediatric Vision Screening For The Family PhysicianDocumento15 páginasPediatric Vision Screening For The Family PhysicianPaula LottiAinda não há avaliações
- RetinoblastomaDocumento45 páginasRetinoblastomaNaide Aulia KudasaiAinda não há avaliações
- Jarvis: Physical Examination & Health Assessment, 3rd Canadian EditionDocumento3 páginasJarvis: Physical Examination & Health Assessment, 3rd Canadian EditionkekeAinda não há avaliações
- About Short-Sightedness .: Normal VisionDocumento5 páginasAbout Short-Sightedness .: Normal VisionSyuhaida AdenanAinda não há avaliações
- Topic Presentation CataractDocumento11 páginasTopic Presentation Cataractjyoti singhAinda não há avaliações
- Research Paper On Night BlindnessDocumento4 páginasResearch Paper On Night Blindnesskbcymacnd100% (1)
- Pediatric Eye Exam Guide for ParentsDocumento14 páginasPediatric Eye Exam Guide for ParentsDrSyed Rahil IqbalAinda não há avaliações
- Congenital Cataract: Call 0303 123 9999 Bringing Together People Affected by Sight LossDocumento22 páginasCongenital Cataract: Call 0303 123 9999 Bringing Together People Affected by Sight Lossswidy fransinAinda não há avaliações
- Congenital Cataracts 2019Documento22 páginasCongenital Cataracts 2019Evy Alvionita YurnaAinda não há avaliações
- Lazy Eye - NHSDocumento1 páginaLazy Eye - NHSNikki HooperAinda não há avaliações
- Breakthrough in Health-GACDocumento25 páginasBreakthrough in Health-GACdolly29100% (1)
- TimRoot - Chapter 7 - Pediatric OphthalmologyDocumento1 páginaTimRoot - Chapter 7 - Pediatric OphthalmologyBaeyerAinda não há avaliações
- MedscapeDocumento12 páginasMedscapeRissa WatlolyAinda não há avaliações
- Biology Investigatory ProjectDocumento19 páginasBiology Investigatory ProjectGopikrishna united67% (3)
- Pediatr Clin Na 2014 Jun 61 (3) 495Documento9 páginasPediatr Clin Na 2014 Jun 61 (3) 495mickymed_Ainda não há avaliações
- Tumor in The EyeDocumento26 páginasTumor in The EyeNor Afira ZaharinAinda não há avaliações
- Cataracts - Causes, Symptoms, Treatment, Surgery: Southern Cross Medical LibraryDocumento6 páginasCataracts - Causes, Symptoms, Treatment, Surgery: Southern Cross Medical Librarypuskesmas sukorejoAinda não há avaliações
- Daftar PustakaDocumento2 páginasDaftar PustakaanggunAinda não há avaliações
- Hepatitis 3Documento12 páginasHepatitis 3anggunAinda não há avaliações
- Daftar Pustaka HepatitisDocumento1 páginaDaftar Pustaka HepatitisanggunAinda não há avaliações
- Growth ChartDocumento8 páginasGrowth ChartanggunAinda não há avaliações
- Dapus 9 - Retinoblastoma and Stimulating LesionsDocumento21 páginasDapus 9 - Retinoblastoma and Stimulating LesionsanggunAinda não há avaliações
- Dapus 15 - RetinoblastomaDocumento4 páginasDapus 15 - RetinoblastomaanggunAinda não há avaliações
- Hepatitis 2Documento4 páginasHepatitis 2Si GeTyAinda não há avaliações
- Lab Manual - Senses Eye - A+p - 2-12-18Documento19 páginasLab Manual - Senses Eye - A+p - 2-12-18Ajit Sinha0% (1)
- Dme C1Documento7 páginasDme C1taliya. shvetzAinda não há avaliações
- Enhancement and Feature Extraction of Fundus ImagesDocumento5 páginasEnhancement and Feature Extraction of Fundus ImagesInternational Journal of Innovative Science and Research TechnologyAinda não há avaliações
- See Without GlassesDocumento144 páginasSee Without Glassesbogdan_1979100% (5)
- Chapter 1 Principles of Confocal Scanning Laser Ophthalmoscopy For The ClinicianDocumento9 páginasChapter 1 Principles of Confocal Scanning Laser Ophthalmoscopy For The ClinicianSaraRosa1992Ainda não há avaliações
- Visual Field Changes in GlaucomaDocumento39 páginasVisual Field Changes in GlaucomaOlayemi OlorundareAinda não há avaliações
- DIP2-Image Processing FundamentalsDocumento47 páginasDIP2-Image Processing FundamentalsMaggieAinda não há avaliações
- Speed of Neural TransmissionDocumento37 páginasSpeed of Neural TransmissionSharon Valerdi LozanoAinda não há avaliações
- Soal TO AAO 12 Dan JawabanDocumento17 páginasSoal TO AAO 12 Dan Jawabancharles indraAinda não há avaliações
- Cilia 2018Documento1 páginaCilia 2018Anna Beatriz Silva EspindolaAinda não há avaliações
- Ocular Complications of Diabetes MellitusDocumento18 páginasOcular Complications of Diabetes MellitusEllieAinda não há avaliações
- RTVue Users Manual Rev 3Documento104 páginasRTVue Users Manual Rev 3Rodrigo Olivares Urbina50% (2)
- Bionic EyeDocumento1 páginaBionic EyesubhasishcAinda não há avaliações
- Eye & Ear Embryology ObjectivesDocumento3 páginasEye & Ear Embryology ObjectivesDr. DAinda não há avaliações
- McCulloch, W. & Pfeiffer, J. of Digital Computers Called BrainsDocumento10 páginasMcCulloch, W. & Pfeiffer, J. of Digital Computers Called BrainsRodolfo van GoodmanAinda não há avaliações
- Diabetic Retinopathy - Practice Essentials, Pathophysiology, EtiologyDocumento11 páginasDiabetic Retinopathy - Practice Essentials, Pathophysiology, EtiologyIrma Kurniawati100% (1)
- UntitledDocumento21 páginasUntitledsweetsalt boyAinda não há avaliações
- Digital Image Fundamentals MCQsDocumento12 páginasDigital Image Fundamentals MCQsSanthosh PaAinda não há avaliações
- X-linked juvenile retinoschisis: Clinical diagnosis, genetic analysis, and molecular mechanismsDocumento18 páginasX-linked juvenile retinoschisis: Clinical diagnosis, genetic analysis, and molecular mechanismsmardocoftAinda não há avaliações
- Week 4 Lab Exercise - Special SensesDocumento12 páginasWeek 4 Lab Exercise - Special SensesJoselito JardielAinda não há avaliações
- Global Wireless e - Voteing SystemDocumento27 páginasGlobal Wireless e - Voteing SystemLaxmi KanthAinda não há avaliações
- Cr-1 Mark II Brochure EnglishDocumento2 páginasCr-1 Mark II Brochure EnglishcwsalesproAinda não há avaliações
- 5 Literature Reader Annexure 187 196 Class XDocumento10 páginas5 Literature Reader Annexure 187 196 Class XAshy Heart HackerAinda não há avaliações
- Santa Monica Institute of Technology: Science 1: Teaching Science in Elementary Grade (Biology and Chemistry)Documento10 páginasSanta Monica Institute of Technology: Science 1: Teaching Science in Elementary Grade (Biology and Chemistry)Chapz PaczAinda não há avaliações
- VETERINARY Techniques of Ophthalmic Examination ManualDocumento29 páginasVETERINARY Techniques of Ophthalmic Examination ManualLuis Torres AlemarAinda não há avaliações
- Automatic Detection of Genetic Diseases in Paediatric Age Using PupillometryDocumento7 páginasAutomatic Detection of Genetic Diseases in Paediatric Age Using PupillometryIJRASETPublicationsAinda não há avaliações
- Bio PhysioDocumento587 páginasBio Physioسامي التريكيAinda não há avaliações
- AP PSYCH CONFUSING PAIRSDocumento7 páginasAP PSYCH CONFUSING PAIRSNam NguyenAinda não há avaliações
- Pearson Science New South Wales 9 Chapter 6 TestDocumento13 páginasPearson Science New South Wales 9 Chapter 6 TestAbigail ScottAinda não há avaliações
- Anatomy of The EyeDocumento3 páginasAnatomy of The EyeNABEEL100% (1)