Você também pode gostar
- Quality Assurance and Quality Control in Neutron Activation Analysis: A Guide to Practical ApproachesNo EverandQuality Assurance and Quality Control in Neutron Activation Analysis: A Guide to Practical ApproachesAinda não há avaliações
- Annual - Report - 11 - 12 2 PDFDocumento11 páginasAnnual - Report - 11 - 12 2 PDFprofarmah6150Ainda não há avaliações
- ICBSE Annual Report 201819 FINALDocumento19 páginasICBSE Annual Report 201819 FINALZaidGoovayAinda não há avaliações
- Annual Report 2011 PDFDocumento10 páginasAnnual Report 2011 PDFprofarmah6150Ainda não há avaliações
- Annual Report 2011Documento10 páginasAnnual Report 2011Mohammed HusseinAinda não há avaliações
- CandidateDocumento42 páginasCandidatemountsAinda não há avaliações
- The Overseas Registration Examination FinalDocumento10 páginasThe Overseas Registration Examination FinalAnonymous geItmk3Ainda não há avaliações
- Https:publishing Rcseng Ac Uk:doi:pdf:10 1308:rcsann 2018 0153Documento7 páginasHttps:publishing Rcseng Ac Uk:doi:pdf:10 1308:rcsann 2018 0153Leonardo Salviano da F RezendeAinda não há avaliações
- Urology Grey ManualDocumento115 páginasUrology Grey ManualdmshossainAinda não há avaliações
- CC M CC M: MM MM MMM M MM MMMM MM MMMM!MMMDocumento31 páginasCC M CC M: MM MM MMM M MM MMMM MM MMMM!MMMFehmidah DsAinda não há avaliações
- Otolaryngology Curriculum Aug 2021 Approved Oct 20Documento117 páginasOtolaryngology Curriculum Aug 2021 Approved Oct 20Amjad AliAinda não há avaliações
- Booklet of Osce InformationDocumento36 páginasBooklet of Osce InformationKatherine Sullivan100% (1)
- MJDF Exam Information PDFDocumento29 páginasMJDF Exam Information PDFAmin HedayatpourAinda não há avaliações
- Exam January 2009 Unit IBDocumento14 páginasExam January 2009 Unit IBlotusracing100% (2)
- OSCE Scope of The OSCE in The Assessment of ClinicDocumento5 páginasOSCE Scope of The OSCE in The Assessment of Clinicdruzair007Ainda não há avaliações
- IMPCB Requirements V10b PDFDocumento35 páginasIMPCB Requirements V10b PDFHilary ChengAinda não há avaliações
- Diploma Guide - EnglishDocumento11 páginasDiploma Guide - EnglishAndra Victoria TitaAinda não há avaliações
- OSCE ManualDocumento40 páginasOSCE Manualdkasis100% (1)
- Regulations & Syllabus: The Royal College of Surgeons of EnglandDocumento26 páginasRegulations & Syllabus: The Royal College of Surgeons of EnglandYousef AlalawiAinda não há avaliações
- SR8 Regulations - OtolaryngologyDocumento4 páginasSR8 Regulations - OtolaryngologyDr-Firas Nayf Al-ThawabiaAinda não há avaliações
- Audit and Clinical Effectiveness Information For OphthalmologistsDocumento12 páginasAudit and Clinical Effectiveness Information For OphthalmologistsHumma ShahidAinda não há avaliações
- Guia para Estudiar para IcoDocumento16 páginasGuia para Estudiar para IcoMaria Silvana Sequera LampeAinda não há avaliações
- Examiners Report Unit D - September 2009 Unit DDocumento10 páginasExaminers Report Unit D - September 2009 Unit DЮрий СиливончикAinda não há avaliações
- Mrcs SyllabusDocumento55 páginasMrcs Syllabussamuelfernando123100% (2)
- Guide To The Intercollegiate MRCS Examination - Singapore 2012Documento55 páginasGuide To The Intercollegiate MRCS Examination - Singapore 2012juweriyAinda não há avaliações
- Anatomy ObeDocumento13 páginasAnatomy ObeRodel AgapitoAinda não há avaliações
- C OphthalDocumento47 páginasC OphthalVissalini JayabalanAinda não há avaliações
- IGC2 Examiner's Reports July - September FinalDocumento14 páginasIGC2 Examiner's Reports July - September Finalمحمد عامرAinda não há avaliações
- Intercollegiate MRCS SyllabusDocumento88 páginasIntercollegiate MRCS Syllabuskelly_ann23Ainda não há avaliações
- Clinical Ophthalmology: Instructions For CandidatesDocumento16 páginasClinical Ophthalmology: Instructions For CandidatesHussain SyedAinda não há avaliações
- MFDS Candidate GuidanceDocumento7 páginasMFDS Candidate Guidancew SMNAinda não há avaliações
- Spiro 7Documento17 páginasSpiro 7Bulborea MihaelaAinda não há avaliações
- Syllabus: Intercollegiate Mrcs Examination MRCS (Ed) (Surgery in General) Oral and ClinicalDocumento88 páginasSyllabus: Intercollegiate Mrcs Examination MRCS (Ed) (Surgery in General) Oral and Clinicalprofarmah6150Ainda não há avaliações
- GeneralguidanceDocumento3 páginasGeneralguidanceMagali EsquivelAinda não há avaliações
- NRE 2023 Dental SyllabusDocumento54 páginasNRE 2023 Dental SyllabusAli Raza Munir AhmadAinda não há avaliações
- LSS EAES Laparoscopic Surgical Skills ProgrammeDocumento8 páginasLSS EAES Laparoscopic Surgical Skills ProgrammeSociedade Portuguesa de Cirurgia100% (1)
- MJDFDocumento2 páginasMJDFKubais Al-Assaf100% (1)
- Oral Surgery Curriculum February 2014 PDFDocumento57 páginasOral Surgery Curriculum February 2014 PDFvipul varmaAinda não há avaliações
- R0194 - Ferramenta de Avaliação de Competências para Suturas Laparoscópicas - Avaliação de Desenvolvimento e Confiabilidade - 2020Documento7 páginasR0194 - Ferramenta de Avaliação de Competências para Suturas Laparoscópicas - Avaliação de Desenvolvimento e Confiabilidade - 2020Sky WingsAinda não há avaliações
- 2013 RCSI Membership Examinations - Middle East (March 2013)Documento5 páginas2013 RCSI Membership Examinations - Middle East (March 2013)ehabmicAinda não há avaliações
- Guide To Application: Chartered Engineer Ceng Chartered Environmentalist Cenv Chartered Scientist CsciDocumento20 páginasGuide To Application: Chartered Engineer Ceng Chartered Environmentalist Cenv Chartered Scientist CsciMuhammad Imran KhanAinda não há avaliações
- MRCS OSCEExam Day Guidance NotesJuly2018CleanDocumento9 páginasMRCS OSCEExam Day Guidance NotesJuly2018CleanShanmuga SundaramAinda não há avaliações
- Frca Final SEC-EXM-FI-ARPT-2013-2014 PDFDocumento9 páginasFrca Final SEC-EXM-FI-ARPT-2013-2014 PDFSuhas KapseAinda não há avaliações
- Surgical Audit and Peer Review Guide 2014Documento54 páginasSurgical Audit and Peer Review Guide 2014juweriyAinda não há avaliações
- MJDF and The Modern: Dental CareerDocumento2 páginasMJDF and The Modern: Dental CareerSarvoday SinhaAinda não há avaliações
- Prospectus - MD and Board Certification in Anaesthesiology 2022Documento189 páginasProspectus - MD and Board Certification in Anaesthesiology 2022Prabhashwara KularathneAinda não há avaliações
- Oral and Maxillofacial SurgeryDocumento49 páginasOral and Maxillofacial SurgeryBhanuSatyanarayanaChowdary100% (1)
- InterMod OMFSDocumento36 páginasInterMod OMFSFahad Qiam75% (4)
- Intercollegiate Surgical Curriculum ENTDocumento98 páginasIntercollegiate Surgical Curriculum ENTMendhi Ashish AnilAinda não há avaliações
- ED1 2009 Exam-Report-Dec PDFDocumento11 páginasED1 2009 Exam-Report-Dec PDFfrancisAinda não há avaliações
- CERTDocumento10 páginasCERTalex ormazabalAinda não há avaliações
- Dental NLE 2021 Syllabus - FinalDocumento55 páginasDental NLE 2021 Syllabus - FinalJohn frostAinda não há avaliações
- Adex Dental Exam Series: Fixed Prosthodontics and EndodonticsDocumento36 páginasAdex Dental Exam Series: Fixed Prosthodontics and EndodonticsmeethaileyyyAinda não há avaliações
- Regulations Effective From January 2017 PDFDocumento13 páginasRegulations Effective From January 2017 PDFash2087Ainda não há avaliações
- Frca Part A SyllabusDocumento91 páginasFrca Part A Syllabushy3pjb1984Ainda não há avaliações
- Dental - Manikin Manual 2021Documento35 páginasDental - Manikin Manual 2021AmariesaAinda não há avaliações
- Guidance Notes For Referees - Generic - Oct 2013Documento2 páginasGuidance Notes For Referees - Generic - Oct 2013syed imdadAinda não há avaliações
- G31 JSCFE Guide To Scope and Format - Otolaryngology 2Documento1 páginaG31 JSCFE Guide To Scope and Format - Otolaryngology 2syed imdadAinda não há avaliações
- Towards best practice in the Archetype Development ProcessNo EverandTowards best practice in the Archetype Development ProcessAinda não há avaliações
- CardiothoracicsurgicallogbookrevisedDocumento8 páginasCardiothoracicsurgicallogbookrevisedprofarmah6150Ainda não há avaliações
- The First Affiliated Hospital of Zhejiang University, ChinaDocumento2 páginasThe First Affiliated Hospital of Zhejiang University, Chinaprofarmah6150Ainda não há avaliações
- Registration PathwayDocumento4 páginasRegistration Pathwayprofarmah6150Ainda não há avaliações
- Chapter 18 - Drug ProblemsDocumento12 páginasChapter 18 - Drug Problemsprofarmah6150Ainda não há avaliações
- For Students and Graduates of Medical Schools in The United States and Canada Accredited by The LCME or AOADocumento1 páginaFor Students and Graduates of Medical Schools in The United States and Canada Accredited by The LCME or AOAprofarmah6150Ainda não há avaliações
- 55 Pain in The Arm and HandsDocumento22 páginas55 Pain in The Arm and Handsprofarmah6150Ainda não há avaliações
- SkillsDocumento2 páginasSkillsprofarmah6150Ainda não há avaliações
- Hey Can I Try ThatDocumento20 páginasHey Can I Try Thatapi-273078602Ainda não há avaliações
- PX4211 2Documento3 páginasPX4211 2kalpanaAinda não há avaliações
- CPC Project PDFDocumento18 páginasCPC Project PDFsiddharthAinda não há avaliações
- ACC 101 - 3rd QuizDocumento3 páginasACC 101 - 3rd QuizAdyangAinda não há avaliações
- University of MauritiusDocumento4 páginasUniversity of MauritiusAtish KissoonAinda não há avaliações
- Asia-Pacific/Arab Gulf Marketscan: Volume 39 / Issue 65 / April 2, 2020Documento21 páginasAsia-Pacific/Arab Gulf Marketscan: Volume 39 / Issue 65 / April 2, 2020Donnie HavierAinda não há avaliações
- GK Test-IiDocumento11 páginasGK Test-IiDr Chaman Lal PTAinda não há avaliações
- Mosaic Charter School TIS Update 12202019Documento73 páginasMosaic Charter School TIS Update 12202019Brandon AtchleyAinda não há avaliações
- BCCA Semester New Syllabus Direction 2016-17 PDFDocumento76 páginasBCCA Semester New Syllabus Direction 2016-17 PDFChetana Gorakh100% (1)
- Cortex - M1: Technical Reference ManualDocumento174 páginasCortex - M1: Technical Reference ManualSzilárd MájerAinda não há avaliações
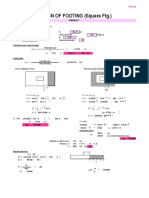
- Design of Footing (Square FTG.) : M Say, L 3.75Documento2 páginasDesign of Footing (Square FTG.) : M Say, L 3.75victoriaAinda não há avaliações
- Ex-Capt. Harish Uppal Vs Union of India & Anr On 17 December, 2002Documento20 páginasEx-Capt. Harish Uppal Vs Union of India & Anr On 17 December, 2002vivek6593Ainda não há avaliações
- Object Based and Unified StorageDocumento12 páginasObject Based and Unified Storageashu narayanAinda não há avaliações
- Pas 1, Presentation of Financial Statements: Philippine Institute of Certified Public AccountantsDocumento38 páginasPas 1, Presentation of Financial Statements: Philippine Institute of Certified Public AccountantsAie GeraldinoAinda não há avaliações
- Thermal Hybrids R5Documento9 páginasThermal Hybrids R5amir.kalantariAinda não há avaliações
- CS 252: Computer Organization and Architecture II: Lecture 5 - The Memory SystemDocumento29 páginasCS 252: Computer Organization and Architecture II: Lecture 5 - The Memory SystemJonnahAinda não há avaliações
- Automatic Star Delta StarterDocumento11 páginasAutomatic Star Delta StarterAmg 360Ainda não há avaliações
- AWS Migrate Resources To New RegionDocumento23 páginasAWS Migrate Resources To New Regionsruthi raviAinda não há avaliações
- C++ & Object Oriented Programming: Dr. Alekha Kumar MishraDocumento23 páginasC++ & Object Oriented Programming: Dr. Alekha Kumar MishraPriyanshu Kumar KeshriAinda não há avaliações
- Anklet - Google SearchDocumento1 páginaAnklet - Google SearchManu KhannaAinda não há avaliações
- Indian Institute of Technology (Indian School of Mines) DhabadDocumento23 páginasIndian Institute of Technology (Indian School of Mines) DhabadAmit KumarAinda não há avaliações
- Group 7 - Mountain DewDocumento18 páginasGroup 7 - Mountain DewRishabh Anand100% (1)
- Siemens Power Engineering Guide 7E 223Documento1 páginaSiemens Power Engineering Guide 7E 223mydearteacherAinda não há avaliações
- A Study of A Skirtless Hovercraft DesignDocumento71 páginasA Study of A Skirtless Hovercraft DesignSunil Kumar P GAinda não há avaliações
- 101 Union of Filipro Employees Vs Vivar (Labor)Documento1 página101 Union of Filipro Employees Vs Vivar (Labor)Kayelyn Lat100% (1)
- Ca50c584 MAYTAGE00011 1 2Documento2 páginasCa50c584 MAYTAGE00011 1 2Michael MartinAinda não há avaliações
- The Application of A Continuous Strip of Woven Material To A Body PartDocumento15 páginasThe Application of A Continuous Strip of Woven Material To A Body Partczeremar chanAinda não há avaliações
- Method Statement For Backfilling WorksDocumento3 páginasMethod Statement For Backfilling WorksCrazyBookWorm86% (7)
- WCN SyllabusDocumento3 páginasWCN SyllabusSeshendra KumarAinda não há avaliações
- Instructions For Comprehensive Exams NovemberDocumento2 páginasInstructions For Comprehensive Exams Novembermanoj reddyAinda não há avaliações