Você também pode gostar
- ECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!No EverandECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!Ainda não há avaliações
- ECG InterpretationDocumento5 páginasECG InterpretationRichelle Dianne Ramos-Giang100% (3)
- ECG/EKG Interpretation: An Easy Approach to Read a 12-Lead ECG and How to Diagnose and Treat ArrhythmiasNo EverandECG/EKG Interpretation: An Easy Approach to Read a 12-Lead ECG and How to Diagnose and Treat ArrhythmiasNota: 5 de 5 estrelas5/5 (2)
- ECG Interpretation Cheat SheetDocumento1 páginaECG Interpretation Cheat Sheethirsi20051879% (24)
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!No EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!Ainda não há avaliações
- ECG InterpretationDocumento95 páginasECG InterpretationShiela Mae Lopez100% (10)
- Electrocardiography in Emergency, Acute, and Critical Care, 2nd EditionNo EverandElectrocardiography in Emergency, Acute, and Critical Care, 2nd EditionNota: 5 de 5 estrelas5/5 (1)
- ECG Mastery Improving Your ECG Interpretation SkillsDocumento23 páginasECG Mastery Improving Your ECG Interpretation SkillsHitesh Deora100% (2)
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsAinda não há avaliações
- EKG ExamplesDocumento9 páginasEKG ExamplesMayer Rosenberg99% (235)
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsAinda não há avaliações
- Recognizing Normal ECGDocumento50 páginasRecognizing Normal ECGJosiephine Bucalon100% (3)
- EKG/ECG Interpretation Made Easy: A Practical Approach to Passing the ECG/EKG Portion of NCLEXNo EverandEKG/ECG Interpretation Made Easy: A Practical Approach to Passing the ECG/EKG Portion of NCLEXNota: 5 de 5 estrelas5/5 (2)
- EKG Pocket GuideDocumento2 páginasEKG Pocket GuideFabian Ramirez HincapiéAinda não há avaliações
- EKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasNo EverandEKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasNota: 3 de 5 estrelas3/5 (5)
- ECG ReadingDocumento11 páginasECG ReadingSuresh Shrestha100% (1)
- Emergency Department Resuscitation of the Critically Ill, 2nd Edition: A Crash Course in Critical CareNo EverandEmergency Department Resuscitation of the Critically Ill, 2nd Edition: A Crash Course in Critical CareAinda não há avaliações
- Basic ECG ReadingDocumento41 páginasBasic ECG ReadingBenj100% (3)
- ECG Rhythm Interpretation 2007Documento533 páginasECG Rhythm Interpretation 2007user123456798100% (20)
- Bonehead Electrocardiography: The Easiest and Best Way to Learn How to Read Electrocardiograms—No Bones About It!No EverandBonehead Electrocardiography: The Easiest and Best Way to Learn How to Read Electrocardiograms—No Bones About It!Nota: 5 de 5 estrelas5/5 (2)
- ArrhythmiaDocumento2 páginasArrhythmiaChris Pritchard93% (30)
- EKG Interpretation: Making EKG/ECG Interpretation Easy!No EverandEKG Interpretation: Making EKG/ECG Interpretation Easy!Ainda não há avaliações
- Ecg Cheat Sheet 35Documento2 páginasEcg Cheat Sheet 35jessjaylee80% (5)
- Cardiac DysrhythmiasDocumento3 páginasCardiac DysrhythmiasKatherine Santiago92% (62)
- Advance Cardiac Life Support: Short, Sweet and to the PointNo EverandAdvance Cardiac Life Support: Short, Sweet and to the PointNota: 3 de 5 estrelas3/5 (2)
- ECG InterpretationDocumento52 páginasECG InterpretationMarcus, RN98% (44)
- EKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationNo EverandEKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationNota: 3 de 5 estrelas3/5 (1)
- ACLS EKG Rhythms and InterpretationDocumento10 páginasACLS EKG Rhythms and Interpretationdonheyzz_02Ainda não há avaliações
- Basic Arrhythmia RulesDocumento3 páginasBasic Arrhythmia Rulesgreenflames0997% (30)
- ECG InterpretationDocumento40 páginasECG InterpretationMuhammad BadrushshalihAinda não há avaliações
- Reading A EKGDocumento10 páginasReading A EKGMayer Rosenberg100% (15)
- Jane Huff ECG Workout Exercises in Arrhythmia Interpretation 2011Documento419 páginasJane Huff ECG Workout Exercises in Arrhythmia Interpretation 2011BiancaPancu90% (40)
- Basic EKG ECG Rhythms CheatsheetDocumento1 páginaBasic EKG ECG Rhythms CheatsheetAhmad83% (6)
- Ecg Made EasyDocumento130 páginasEcg Made EasyJOHN ARBIE TATTAO, RN96% (49)
- Dysrhythmias ChartDocumento6 páginasDysrhythmias Chartjkrix100% (1)
- Basic ECG and Arrhythmia FINALDocumento16 páginasBasic ECG and Arrhythmia FINALCharlotte James100% (5)
- Cardiac Dysrhythmia Chart Med-Surg NUR4Documento3 páginasCardiac Dysrhythmia Chart Med-Surg NUR4ktfosterfd2096% (97)
- With A Pulse and Poor Perfusion: Pediatric TachycardiaDocumento1 páginaWith A Pulse and Poor Perfusion: Pediatric TachycardiaIin-Ignasia Diahayujulindah Mujiman0% (1)
- NCM 112 MSN Prelim Topic 4 Cardiac Rhythm DisordersDocumento5 páginasNCM 112 MSN Prelim Topic 4 Cardiac Rhythm DisordersKim Erida QuezonAinda não há avaliações
- Assess Appropriateness For Clinical Condition. Heart Rate Typically 150/min If TachyarrhythmiaDocumento1 páginaAssess Appropriateness For Clinical Condition. Heart Rate Typically 150/min If TachyarrhythmiaSiti Nur R Firda FauziyahAinda não há avaliações
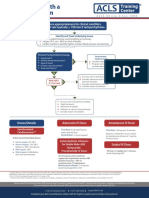
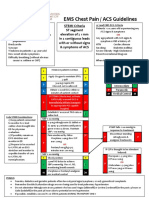
- EMS Chest Pain / ACS GuidelinesDocumento1 páginaEMS Chest Pain / ACS GuidelinesJuanaly BadiolaAinda não há avaliações
- Format in Drug StudyDocumento14 páginasFormat in Drug StudyShenielyn Bartolome NapolitanoAinda não há avaliações
- G2015 Adult Tachycardia PDFDocumento1 páginaG2015 Adult Tachycardia PDFPlabber JuneAinda não há avaliações
- G2015 Adult Tachycardia PDFDocumento1 páginaG2015 Adult Tachycardia PDFibbs91Ainda não há avaliações
- AdultTachycardiaWithPulse AlgorithmDocumento1 páginaAdultTachycardiaWithPulse AlgorithmIsmail SlimAinda não há avaliações
- ACLS Algorithm Pulse No Yes: Stable Patient Unstable Patient Stable PatientDocumento1 páginaACLS Algorithm Pulse No Yes: Stable Patient Unstable Patient Stable PatientAhmed AlkhaqaniAinda não há avaliações
- Peri-Arrest ArrythmiaDocumento14 páginasPeri-Arrest Arrythmiamohamed mowafeyAinda não há avaliações
- Drug Study ErDocumento3 páginasDrug Study ErZheyrille A. ArevaloAinda não há avaliações
- Simplified ACLS AlgorithmDocumento1 páginaSimplified ACLS AlgorithmBrianAinda não há avaliações
- Critical Care Drug Reference SheetDocumento12 páginasCritical Care Drug Reference SheetYanina CoxAinda não há avaliações
- Drug StudyDocumento5 páginasDrug Studyeduardbaldoz69Ainda não há avaliações
- Drug 3Documento8 páginasDrug 3Lorenzo LiteAinda não há avaliações
- Sinus Bradycardia: o No TX If AsymptomaticDocumento3 páginasSinus Bradycardia: o No TX If Asymptomaticelle50% (2)
- ACLS Drug Therapy RevisedDocumento4 páginasACLS Drug Therapy RevisedpaveethrahAinda não há avaliações
- Generic Name: Action: Indications: Adverse Effects:: Injection, OTC Nasal SolutionDocumento20 páginasGeneric Name: Action: Indications: Adverse Effects:: Injection, OTC Nasal SolutionBhupesh PatidarAinda não há avaliações
- Mind Maping MIDocumento1 páginaMind Maping MIimambiyono9728Ainda não há avaliações
- EpinephrineDocumento1 páginaEpinephrineGreshil Castro IgtanlocAinda não há avaliações
- Community Data AssessmentDocumento1 páginaCommunity Data AssessmentAnton LaurencianaAinda não há avaliações
- Ecg ReadingsDocumento11 páginasEcg ReadingsAnton Laurenciana100% (5)
- Zika VirusDocumento2 páginasZika VirusAnton LaurencianaAinda não há avaliações
- Intro Research Study IIDocumento1 páginaIntro Research Study IIAnton LaurencianaAinda não há avaliações
- B1 CHNNCPDocumento5 páginasB1 CHNNCPAnton LaurencianaAinda não há avaliações
- Nada de Util Frequency RateDocumento1 páginaNada de Util Frequency RateGabriel L.G. DivinoAinda não há avaliações
- Plan of CareDocumento4 páginasPlan of CareAnton LaurencianaAinda não há avaliações
- Cholecystitis Case PresDocumento103 páginasCholecystitis Case PresAnton LaurencianaAinda não há avaliações
- Topic Outline OF Functional Health Pattern Assessment: Early ChildhoodDocumento3 páginasTopic Outline OF Functional Health Pattern Assessment: Early ChildhoodAnton LaurencianaAinda não há avaliações
- 2nd Edited Chapter 2-Definition and History of Psychological First Aid1Documento2 páginas2nd Edited Chapter 2-Definition and History of Psychological First Aid1Anton LaurencianaAinda não há avaliações
- Developing Structured SelfDocumento2 páginasDeveloping Structured SelfAnton LaurencianaAinda não há avaliações
- Behavioral Analysis FinalDocumento186 páginasBehavioral Analysis FinalAnton LaurencianaAinda não há avaliações
- Tidal ModelDocumento2 páginasTidal ModelAnton LaurencianaAinda não há avaliações
- Pathophysiologyprostate CADocumento3 páginasPathophysiologyprostate CAAnton LaurencianaAinda não há avaliações
- Multiple Physical Injuries Secondary To Vehicular AccidentDocumento31 páginasMultiple Physical Injuries Secondary To Vehicular AccidentAnton Laurenciana50% (2)
- Chest Trauma Concept MapDocumento10 páginasChest Trauma Concept MapAnton Laurenciana100% (1)
- Chest Trauma RuDocumento37 páginasChest Trauma RuAnton Laurenciana100% (1)
- Heart Disease in PregnancyDocumento33 páginasHeart Disease in PregnancyKanishka KonarAinda não há avaliações
- ACLS Algorithms SlideDocumento26 páginasACLS Algorithms SlidehrsoAinda não há avaliações
- ECG Rhythm Interpretation: How To Analyze A RhythmDocumento12 páginasECG Rhythm Interpretation: How To Analyze A RhythmsrimatsimhasaneshwarAinda não há avaliações
- ESC Guidelines For The Diagnosis and Treatment of Chronic Heart FailureDocumento26 páginasESC Guidelines For The Diagnosis and Treatment of Chronic Heart FailureNareshiman SubramaniamAinda não há avaliações
- Rangkuman ECHODocumento6 páginasRangkuman ECHOwinAinda não há avaliações
- Holter Monitor RedactedDocumento11 páginasHolter Monitor RedactedAnonymous f2WeA3Ainda não há avaliações
- Essentials of Operative Cardiac SurgeryDocumento134 páginasEssentials of Operative Cardiac SurgeryJan CoveliersAinda não há avaliações
- Association of Serum Magnesium On Mortality in Patients Admitted To The Intensive Cardiac Care UnitDocumento9 páginasAssociation of Serum Magnesium On Mortality in Patients Admitted To The Intensive Cardiac Care UnitDr Mohammed Nizam UddinAinda não há avaliações
- Radcliffe EducationDocumento4 páginasRadcliffe EducationSherwin Buenavente SulitAinda não há avaliações
- F4AECCF9 - PBL Week 4 KidneyDocumento13 páginasF4AECCF9 - PBL Week 4 KidneyKahfi AzzumardiAinda não há avaliações
- Family Medicine Study GuideDocumento240 páginasFamily Medicine Study GuideJeremy Christmann100% (1)
- Acute ST Elevation Myocardial Infarction - StatPearls - NCBI BookshelfDocumento9 páginasAcute ST Elevation Myocardial Infarction - StatPearls - NCBI BookshelfZ Siclayi AtlAinda não há avaliações
- Hepato and Cardiorenal SyndromeDocumento31 páginasHepato and Cardiorenal SyndromeanandababuAinda não há avaliações
- The Sample of PediatricsDocumento47 páginasThe Sample of PediatricsWaseem UllahAinda não há avaliações
- Toate Bolile CardiovasculareDocumento6 páginasToate Bolile CardiovasculareAnca CopreanAinda não há avaliações
- High Yield Cardiology Internal Medicine Shelf PDFDocumento44 páginasHigh Yield Cardiology Internal Medicine Shelf PDFsaja fuadAinda não há avaliações
- ECG Monitoring in TheatreDocumento17 páginasECG Monitoring in TheatrePhani NadellaAinda não há avaliações
- IFU Ed 2.0 - DFM100 - English-453564403811Documento240 páginasIFU Ed 2.0 - DFM100 - English-453564403811technicalservice.pnpAinda não há avaliações
- Resident/Fellow Member Application: CodeDocumento2 páginasResident/Fellow Member Application: CodeKavya ShreeAinda não há avaliações
- L1 - SyncopeDocumento5 páginasL1 - SyncopeMuthukumaranAinda não há avaliações
- Congenital Heart DiseaseDocumento124 páginasCongenital Heart DiseasemulkanmustafaAinda não há avaliações
- MIDocumento22 páginasMIGagauz SiliviaAinda não há avaliações
- File Asli Jurnal Panthofisiology Heart FailureDocumento12 páginasFile Asli Jurnal Panthofisiology Heart FailureFitrotur RachmaAinda não há avaliações
- 7.1 Monitoring, Rhythm Recognition, 12-Lead ECG Guidance 2010Documento3 páginas7.1 Monitoring, Rhythm Recognition, 12-Lead ECG Guidance 2010brianed231Ainda não há avaliações
- Catheter Ablation For Atrial Fibrillation: Original ArticleDocumento7 páginasCatheter Ablation For Atrial Fibrillation: Original ArticleGavin WinkelAinda não há avaliações
- SL Penyakit Jantung Pulmonal & HipertensiDocumento24 páginasSL Penyakit Jantung Pulmonal & HipertensiReni MelindaAinda não há avaliações
- AY Unstable Angina PectorisDocumento24 páginasAY Unstable Angina PectorisaybatariAinda não há avaliações
- Circulatory System Diseases QuizDocumento3 páginasCirculatory System Diseases QuizMaruja RuizAinda não há avaliações
- IntroductionDocumento4 páginasIntroductionCristina L. JaysonAinda não há avaliações
- Unstable Angina PectorisDocumento34 páginasUnstable Angina PectoriserinmowokaAinda não há avaliações