Você também pode gostar
- Pre-Employment Medical ExaminationDocumento4 páginasPre-Employment Medical ExaminationRohit Chaudhary100% (1)
- Bidaa Tower Risk Assessment From CALISTO UpdatedDocumento5 páginasBidaa Tower Risk Assessment From CALISTO Updatedirshad gAinda não há avaliações
- Working at Same Levels (High Risk Areas) RA-R9-01-001-02Documento1 páginaWorking at Same Levels (High Risk Areas) RA-R9-01-001-02cmrig74Ainda não há avaliações
- AP Medical ReportDocumento3 páginasAP Medical ReportKatia KatiaAinda não há avaliações
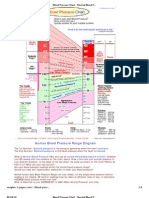
- Blood Pressure ChartDocumento4 páginasBlood Pressure ChartPixelateAinda não há avaliações
- Urgentcare FormDocumento4 páginasUrgentcare Formapi-287654333Ainda não há avaliações
- Medical History and Evaluation FormDocumento22 páginasMedical History and Evaluation FormJobelle Fernandez-SantosAinda não há avaliações
- Risk Assessment for Scaffolding WorkDocumento5 páginasRisk Assessment for Scaffolding WorkAejaz MujawarAinda não há avaliações
- Medical Certificate of Fitness: Section 1: Candidate's Personal DetailsDocumento2 páginasMedical Certificate of Fitness: Section 1: Candidate's Personal DetailsSwastik Trading AgenciesAinda não há avaliações
- Risk Assessment: Being Safe: Example CalculationDocumento2 páginasRisk Assessment: Being Safe: Example CalculationMarcelo RochaAinda não há avaliações
- Consent For Release of Medical RecordsDocumento1 páginaConsent For Release of Medical RecordsCarrboro Family MedicineAinda não há avaliações
- Risk Assessment For SLAB ON GRADE Work: Initial Risk Score Control Measure Residual Risk Score Action VerifiedDocumento2 páginasRisk Assessment For SLAB ON GRADE Work: Initial Risk Score Control Measure Residual Risk Score Action Verifiedeng mohamad husamAinda não há avaliações
- Clinical Health RequirementsDocumento6 páginasClinical Health RequirementsbarneylovesbagelsAinda não há avaliações
- Post Traumatic Stress Disorder (PTSD)Documento4 páginasPost Traumatic Stress Disorder (PTSD)Samreen Jawaid100% (1)
- Sample of JHA - Roofing Top Installation Rev 2Documento5 páginasSample of JHA - Roofing Top Installation Rev 2vajiravel407Ainda não há avaliações
- INCIDENT REPORT FORMDocumento2 páginasINCIDENT REPORT FORMMoumitaAinda não há avaliações
- 01 WI HSE 001 - Risk Assessment BridgesDocumento8 páginas01 WI HSE 001 - Risk Assessment BridgesMisbah Ul Haq LabeedAinda não há avaliações
- Medical exam form summaryDocumento4 páginasMedical exam form summaryAldwin Bagtas0% (1)
- 3384 SWM Ergonomic Risk Factor Checklist1Documento5 páginas3384 SWM Ergonomic Risk Factor Checklist1Anonymous V2HS9gtFAinda não há avaliações
- FCU Quarterly PPM: Risk Assessment (Ra) FormDocumento2 páginasFCU Quarterly PPM: Risk Assessment (Ra) FormRAJ CHAUDHARYAinda não há avaliações
- Employee Medical Incident ReportDocumento1 páginaEmployee Medical Incident ReportAiswarya SukumarAinda não há avaliações
- (Sample) Completion of Works CertificateDocumento1 página(Sample) Completion of Works CertificateFredrick Omondi OleweAinda não há avaliações
- Fit For Duty Work Policy Short FormDocumento3 páginasFit For Duty Work Policy Short FormSunish RathaurAinda não há avaliações
- TOOLBOX FatigueDocumento36 páginasTOOLBOX FatigueGilbert Antoni QuirogaAinda não há avaliações
- Hospital Referral FormDocumento1 páginaHospital Referral FormNether MonsterAinda não há avaliações
- Medical Fitness CertificateDocumento2 páginasMedical Fitness CertificatePraveen Kumar Madupu100% (1)
- Accident ReportingDocumento26 páginasAccident ReportinggerryfmarrAinda não há avaliações
- Certificate of FitnessDocumento2 páginasCertificate of FitnessKarthik SAinda não há avaliações
- Fitness For WorkDocumento13 páginasFitness For WorkPABLO HUGO CEVALLOS ALEGRIAAinda não há avaliações
- Confined Space Risk Assessment WHSFOR-009BDocumento3 páginasConfined Space Risk Assessment WHSFOR-009BvictorAinda não há avaliações
- Adult Health HistoryDocumento1 páginaAdult Health HistorySally Hansen100% (1)
- Fitness For Work PolicyDocumento2 páginasFitness For Work Policyjaultry muhuyiAinda não há avaliações
- Risk Assessment Template: Step 1: Identify The HazardsDocumento4 páginasRisk Assessment Template: Step 1: Identify The HazardsMyolwinooAinda não há avaliações
- Records ReleaseDocumento1 páginaRecords ReleasechelseaAinda não há avaliações
- Report of An Injury or Dangerous Occurrence: Part A Part CDocumento2 páginasReport of An Injury or Dangerous Occurrence: Part A Part CVeronica Navarro CorbiAinda não há avaliações
- HPV Vaccine Powerpoint PresentationDocumento18 páginasHPV Vaccine Powerpoint Presentationkristia destiAinda não há avaliações
- Health and Safety Management in HealthcareDocumento6 páginasHealth and Safety Management in HealthcareDr.ManageAinda não há avaliações
- Science of Self RealizationDocumento343 páginasScience of Self Realizationapi-3699487100% (1)
- Medical Certificate of Fitness-2Documento2 páginasMedical Certificate of Fitness-2Shishir MathurAinda não há avaliações
- New Patient FormDocumento4 páginasNew Patient Formapi-288684181Ainda não há avaliações
- First Aid and Wound Care2Documento24 páginasFirst Aid and Wound Care2Clowitzky IsikAinda não há avaliações
- Dispersion Modeling 101Documento32 páginasDispersion Modeling 101Krishna SrikanthAinda não há avaliações
- CD-42 - Medical QuestionnaireDocumento6 páginasCD-42 - Medical QuestionnaireRasLDKAinda não há avaliações
- Employees Accedent ReportDocumento1 páginaEmployees Accedent ReportKomal TiwariAinda não há avaliações
- Best Practices in ESP Operation and Maintenance For Improved PerformanceDocumento6 páginasBest Practices in ESP Operation and Maintenance For Improved PerformanceRanjan PalAinda não há avaliações
- Na Aqs Manual Volume IDocumento62 páginasNa Aqs Manual Volume IKutticad RameshAinda não há avaliações
- Is 9989 1981Documento18 páginasIs 9989 1981Krishna SrikanthAinda não há avaliações
- Incident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ADocumento2 páginasIncident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ARocky BisAinda não há avaliações
- CBC 2013 WaiverandRelease Minor FormDocumento1 páginaCBC 2013 WaiverandRelease Minor FormCory James HutchersonAinda não há avaliações
- Medical CertificateDocumento2 páginasMedical CertificatelekacaAinda não há avaliações
- Job Safety Analysis 0Documento6 páginasJob Safety Analysis 0Edi Gunawan BanjarnahorAinda não há avaliações
- MOHE Health Declaration and Medical Examination FormDocumento5 páginasMOHE Health Declaration and Medical Examination Formnazrin sarajuddinAinda não há avaliações
- Work Shop TRA AC Maintenance 01Documento15 páginasWork Shop TRA AC Maintenance 01Tarik MunafAinda não há avaliações
- Form-12 Accident Report From EmployerDocumento2 páginasForm-12 Accident Report From Employersupriya100% (2)
- Transcript of The Videotelephony Medical Examination ReportDocumento2 páginasTranscript of The Videotelephony Medical Examination ReportKamarapu Vamshee KrishnaAinda não há avaliações
- 4 16 Employment Employment ContractDocumento6 páginas4 16 Employment Employment ContractDimol Sedoc 10 G2Ainda não há avaliações
- Hazard Identification Risk Assessment Risk Control (HIRARC) FormDocumento1 páginaHazard Identification Risk Assessment Risk Control (HIRARC) FormJeft TanAinda não há avaliações
- Tool Box Talk - Working in Hot WeatherDocumento1 páginaTool Box Talk - Working in Hot WeatherMobashir MahmoodAinda não há avaliações
- Hso Medical Examination FormDocumento2 páginasHso Medical Examination FormKhoirul FikriAinda não há avaliações
- A Guide To Selecting Non-Powered Hand Tools: Easy ErgonomicsDocumento20 páginasA Guide To Selecting Non-Powered Hand Tools: Easy ErgonomicsLibyaFlowerAinda não há avaliações
- Stemi ChecklistDocumento1 páginaStemi ChecklistDanu SusantoAinda não há avaliações
- Injury Report FormDocumento2 páginasInjury Report FormFrank Abuda100% (2)
- Accident Report FormDocumento5 páginasAccident Report Formyenni mirandaAinda não há avaliações
- Incident Investigation Report FormDocumento7 páginasIncident Investigation Report FormAlexis MillsAinda não há avaliações
- Lamp Sesi 8.2 Investigasi SCATDocumento2 páginasLamp Sesi 8.2 Investigasi SCATaab kanayaAinda não há avaliações
- Bio-Medical Waste Management - Fee Structure - Andhra Pradesh Pollution Control Board - APPCBDocumento3 páginasBio-Medical Waste Management - Fee Structure - Andhra Pradesh Pollution Control Board - APPCBKrishna SrikanthAinda não há avaliações
- Is 5182 10 1999Documento15 páginasIs 5182 10 1999Krishna SrikanthAinda não há avaliações
- Frequently Asked Questions (FAQ) On Wastewater - Sewage Treatment Plants (STP)Documento11 páginasFrequently Asked Questions (FAQ) On Wastewater - Sewage Treatment Plants (STP)Krishna SrikanthAinda não há avaliações
- Low Carbon Life StylesDocumento28 páginasLow Carbon Life StylesSaurav RukhaiyarAinda não há avaliações
- 2-Earth Composition StructureDocumento34 páginas2-Earth Composition StructureDarsRayAinda não há avaliações
- 2-Earth Composition StructureDocumento34 páginas2-Earth Composition StructureDarsRayAinda não há avaliações
- Air Pollution Control A Design ApproachDocumento427 páginasAir Pollution Control A Design ApproachKY TianaAinda não há avaliações
- Healthy Nutrition - National Health Portal of IndiaDocumento10 páginasHealthy Nutrition - National Health Portal of IndiaKrishna SrikanthAinda não há avaliações
- 25 Ways To Improve Your Life - Sri Sri RavishankarDocumento14 páginas25 Ways To Improve Your Life - Sri Sri RavishankarSreeraj Guruvayoor SAinda não há avaliações
- Guidelines For Real Time Sampling & Analyses: Guidelines For The Measurement of Ambient Air PollutantsDocumento54 páginasGuidelines For Real Time Sampling & Analyses: Guidelines For The Measurement of Ambient Air PollutantsnayancoepmechAinda não há avaliações
- ENVIRONMENTAL COMPLIANCEDocumento7 páginasENVIRONMENTAL COMPLIANCEKrishna SrikanthAinda não há avaliações
- Perfect Questions Perfect AnswersDocumento40 páginasPerfect Questions Perfect AnswersGopalaGuruAinda não há avaliações
- Thermal Power Plant StandardsDocumento5 páginasThermal Power Plant StandardsKrishna SrikanthAinda não há avaliações
- Cholesterol FactsDocumento3 páginasCholesterol FactssureshjeevaAinda não há avaliações
- Cholesterol FactsDocumento3 páginasCholesterol FactssureshjeevaAinda não há avaliações
- Safety Sign 1750379Documento1 páginaSafety Sign 1750379Krishna SrikanthAinda não há avaliações
- Disclosure To Promote The Right To InformationDocumento15 páginasDisclosure To Promote The Right To InformationKrishna SrikanthAinda não há avaliações
- Carbon FootprintDocumento9 páginasCarbon FootprintKrishna SrikanthAinda não há avaliações
- Stack Monitoring-Feb 19Documento18 páginasStack Monitoring-Feb 19Krishna SrikanthAinda não há avaliações
- B Ipi CH 2010 4 14Documento12 páginasB Ipi CH 2010 4 14Krishna SrikanthAinda não há avaliações
- Annexure I: National Ambient Air Quality Standards - NewDocumento5 páginasAnnexure I: National Ambient Air Quality Standards - NewKrishna SrikanthAinda não há avaliações
- Lit - Pure Water HandbookDocumento151 páginasLit - Pure Water HandbookGreg ReynekeAinda não há avaliações
- Chemical Engineering Objective Type Questions SedimentationDocumento5 páginasChemical Engineering Objective Type Questions SedimentationKrishna Srikanth0% (1)