Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Hollie Poe Summer 2016 Research Paper GynecomastiaDocumento14 páginasHollie Poe Summer 2016 Research Paper Gynecomastiaapi-349402240Ainda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Clinical Totals 2Documento1 páginaClinical Totals 2api-349402240Ainda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Clinical TotalsDocumento1 páginaClinical Totalsapi-349402240Ainda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Renal Doppler Protocol 14 1Documento4 páginasRenal Doppler Protocol 14 1api-349402240100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Female Pelvis Protocol r16 1Documento2 páginasFemale Pelvis Protocol r16 1api-349402240Ainda não há avaliações
- Clinical EvaluationsDocumento1 páginaClinical Evaluationsapi-349402240Ainda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Upper Extremity Venous Protocol 14Documento2 páginasUpper Extremity Venous Protocol 14api-349402240Ainda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Hepatic Doppler Protocol 14Documento4 páginasHepatic Doppler Protocol 14api-349402240Ainda não há avaliações
- Pediatric Spine 14Documento2 páginasPediatric Spine 14api-349402240Ainda não há avaliações
- Upper Extremity Arterial Protocol 14Documento3 páginasUpper Extremity Arterial Protocol 14api-349402240Ainda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Lower Extremity Venous Protocol 14Documento3 páginasLower Extremity Venous Protocol 14api-349474075Ainda não há avaliações
- Lower Extremity Venous Incompetence Protcol 14Documento5 páginasLower Extremity Venous Incompetence Protcol 14api-349402240Ainda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Mesenteric Doppler Protocol 14Documento2 páginasMesenteric Doppler Protocol 14api-349402240Ainda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Thoracic Outlet Syndrome Protocol 14Documento2 páginasThoracic Outlet Syndrome Protocol 14api-349402240Ainda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Lower Extremity Arterial Protocol 14 1Documento2 páginasLower Extremity Arterial Protocol 14 1api-3494022400% (1)
- Allen Test Protocol 14 1Documento2 páginasAllen Test Protocol 14 1api-349402240Ainda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
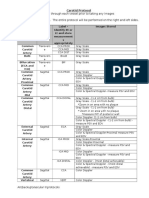
- Carotid Protocol 14 1Documento4 páginasCarotid Protocol 14 1api-349402240Ainda não há avaliações
- Breast Protocol 14 1Documento4 páginasBreast Protocol 14 1api-349402240Ainda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Thyroid Protocol 14 1Documento3 páginasThyroid Protocol 14 1api-349402240Ainda não há avaliações
- Neonatal Head Protocol 14Documento5 páginasNeonatal Head Protocol 14api-349402240Ainda não há avaliações
- Pyloric Stenosis 14Documento3 páginasPyloric Stenosis 14api-349402240Ainda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Scrotum Protocol 14Documento2 páginasScrotum Protocol 14api-349402240Ainda não há avaliações
- Pediatric Hip Protocol 14Documento3 páginasPediatric Hip Protocol 14api-349402240Ainda não há avaliações
- Urinary Protocol 14 1Documento4 páginasUrinary Protocol 14 1api-349402240Ainda não há avaliações
- Pancreas Protocol 14 2Documento2 páginasPancreas Protocol 14 2api-349402240Ainda não há avaliações
- Fetal Echocardiogram ProtocolDocumento4 páginasFetal Echocardiogram Protocolapi-349402240Ainda não há avaliações
- Adult Echocardiography Protocol 14 2Documento10 páginasAdult Echocardiography Protocol 14 2api-349402240Ainda não há avaliações
- Abdomen ProtocolDocumento8 páginasAbdomen Protocolapi-349474075Ainda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Prostate Protocol 14 1Documento3 páginasProstate Protocol 14 1api-349402240Ainda não há avaliações
- Feldenkrais®: & The BrainDocumento9 páginasFeldenkrais®: & The BrainPhytodoc0% (1)
- Blood Rhe Ology and Hemo DynamicsDocumento16 páginasBlood Rhe Ology and Hemo Dynamicsandrei_mititeluAinda não há avaliações
- Lower Mandible Maneuver and Elite SingersDocumento20 páginasLower Mandible Maneuver and Elite SingersBryan ChenAinda não há avaliações
- Sexual JealousyDocumento11 páginasSexual JealousyLip Stick100% (1)
- Glucose Control Solution: Lifescan Healthcare Professional LineDocumento2 páginasGlucose Control Solution: Lifescan Healthcare Professional LineChiehgriffin LaiAinda não há avaliações
- AIIMS May 2019 - PhysiologyDocumento3 páginasAIIMS May 2019 - Physiologyshibira surendran vkAinda não há avaliações
- Bhakti Warrior Teacher Training: Perspectives On Prana and Energetic AnatomyDocumento57 páginasBhakti Warrior Teacher Training: Perspectives On Prana and Energetic AnatomyStuart Rice100% (6)
- The Split Brain in ManDocumento6 páginasThe Split Brain in ManAKISAinda não há avaliações
- Acei and ArbDocumento6 páginasAcei and ArbNurulrezki AtikaAinda não há avaliações
- Chloroplast: Chloroplast-The Site of PhotosynthesisDocumento2 páginasChloroplast: Chloroplast-The Site of PhotosynthesisDrRuby Ranjan SharmaAinda não há avaliações
- L6 8ca Respiration AAFDocumento15 páginasL6 8ca Respiration AAFalirazanqvi310Ainda não há avaliações
- Doppler Artifacts and PitfallsDocumento31 páginasDoppler Artifacts and PitfallsButton Davidson100% (1)
- C-Phycocyanin Powder ChemxpertDocumento11 páginasC-Phycocyanin Powder Chemxpertbalwant chemxpertAinda não há avaliações
- Kera Ritual Menu - With DensifiqueDocumento8 páginasKera Ritual Menu - With Densifiquee.K.e.kAinda não há avaliações
- Corail Surgical Technique Revision 1Documento20 páginasCorail Surgical Technique Revision 1Kaustubh KeskarAinda não há avaliações
- Cardiac Physiology NotesDocumento11 páginasCardiac Physiology Notespunter11100% (1)
- Njala University CHO BSC Level 200Documento6 páginasNjala University CHO BSC Level 200Mathew Moinina SonnieAinda não há avaliações
- Cytokines, Cytokine Receptors and Chemokines: Sept. 11, 2014Documento101 páginasCytokines, Cytokine Receptors and Chemokines: Sept. 11, 2014ANJU0709Ainda não há avaliações
- Hyper Bilirubin Emi ADocumento36 páginasHyper Bilirubin Emi ASai Krishna MaddiralaAinda não há avaliações
- Protein Characterization/Purification: Dr. Kevin AhernDocumento34 páginasProtein Characterization/Purification: Dr. Kevin AhernkelpachurpaAinda não há avaliações
- Third Stage Complications and Post-Partum CollapseDocumento44 páginasThird Stage Complications and Post-Partum CollapseRamlah Ibrahim100% (1)
- Cardiac ArrestDocumento30 páginasCardiac ArrestTommy NainggolanAinda não há avaliações
- ECG Notes Interpretation and ManagementDocumento235 páginasECG Notes Interpretation and ManagementRifQi Kurniawan100% (9)
- Brainstem Medulla Pons MidbrainDocumento3 páginasBrainstem Medulla Pons MidbrainAngela HabaradasAinda não há avaliações
- Biochem Rev Chap 8Documento3 páginasBiochem Rev Chap 8Jacob PallorinaAinda não há avaliações
- Diagnosis, Treatment, Follow Up CTSDocumento11 páginasDiagnosis, Treatment, Follow Up CTSRamjoAinda não há avaliações
- Trans Clinical Chemistry Lec4Documento10 páginasTrans Clinical Chemistry Lec4Kelvin CafirmaAinda não há avaliações
- (Oxy) Med-Surg Checklist With RationaleDocumento13 páginas(Oxy) Med-Surg Checklist With RationaleUri Perez MontedeRamos100% (1)
- Equ211-01 Siemens Dimension Fast FactsDocumento26 páginasEqu211-01 Siemens Dimension Fast Factsmagendi indra muktiAinda não há avaliações
- PPE Physical Exam Form Single PageDocumento1 páginaPPE Physical Exam Form Single PageyumminAinda não há avaliações
- The Age of Magical Overthinking: Notes on Modern IrrationalityNo EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityNota: 4 de 5 estrelas4/5 (29)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDNo EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDNota: 5 de 5 estrelas5/5 (2)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsAinda não há avaliações
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNo EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNota: 4 de 5 estrelas4/5 (404)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNo EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNota: 5 de 5 estrelas5/5 (81)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNo EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNota: 3.5 de 5 estrelas3.5/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsNo EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsNota: 4.5 de 5 estrelas4.5/5 (170)