Você também pode gostar
- Endodontic RadiologyNo EverandEndodontic RadiologyBettina BasraniAinda não há avaliações
- Fixed Orthodontic Appliances: A Practical GuideNo EverandFixed Orthodontic Appliances: A Practical GuideNota: 1 de 5 estrelas1/5 (1)
- The Effectiveness of Auxiliary Features On A Tooth Preparation With Inadequate Resistance FormDocumento9 páginasThe Effectiveness of Auxiliary Features On A Tooth Preparation With Inadequate Resistance FormJhon Anderson Buendìa GarcìaAinda não há avaliações
- Clinical Applications of Digital Dental TechnologyDocumento397 páginasClinical Applications of Digital Dental TechnologyTheo_96Ainda não há avaliações
- Endodontic Course Guidebook 2012 Year 3Documento50 páginasEndodontic Course Guidebook 2012 Year 3Wan NoorinaAinda não há avaliações
- Pulp Therapy For Primary and Immature Permanent TeethDocumento11 páginasPulp Therapy For Primary and Immature Permanent TeethPrabhjot KaurAinda não há avaliações
- Jung 2018Documento11 páginasJung 2018Sebastien MelloulAinda não há avaliações
- Journal ClubDocumento2 páginasJournal ClubWaseem AhmedAinda não há avaliações
- Literature GuideDocumento60 páginasLiterature Guide12345sagarAinda não há avaliações
- Endo LaseDocumento5 páginasEndo LaseAlex PaunAinda não há avaliações
- Overseas Registration Examination Reading ListDocumento3 páginasOverseas Registration Examination Reading ListyoAinda não há avaliações
- Antibiotic Prophylaxis in DentistryDocumento9 páginasAntibiotic Prophylaxis in DentistryLiana OpriţăAinda não há avaliações
- Reducing The Risk of Failure Incomplete Denture PatientsDocumento8 páginasReducing The Risk of Failure Incomplete Denture PatientsHisyam IshakAinda não há avaliações
- Complications of Exodontics: Mary Cris P EstandarteDocumento49 páginasComplications of Exodontics: Mary Cris P EstandarteRealyn D. BerderaAinda não há avaliações
- An Alternative Treatment Approach To Gingival Recession: Gingiva-Colored Partial Porcelain Veneers: A Clinical ReportDocumento22 páginasAn Alternative Treatment Approach To Gingival Recession: Gingiva-Colored Partial Porcelain Veneers: A Clinical ReportSoumya Promod100% (1)
- Introduction To ProsthodonticsDocumento98 páginasIntroduction To ProsthodonticsmarwaAinda não há avaliações
- Seminar TopicsDocumento1 páginaSeminar TopicsDadi SindhuAinda não há avaliações
- Rethinking FerruleDocumento10 páginasRethinking FerruleteodudeAinda não há avaliações
- Properties of Calcihydroxide in TicDocumento34 páginasProperties of Calcihydroxide in TicPhạm CườngAinda não há avaliações
- Wear of Teeth and RestorationsDocumento7 páginasWear of Teeth and RestorationsAya Ibrahim YassinAinda não há avaliações
- Extrac 1Documento49 páginasExtrac 1api-19916399Ainda não há avaliações
- Copy Dentures: Presenter DR Obiero Moderator DR Omondi 2/3/2021Documento58 páginasCopy Dentures: Presenter DR Obiero Moderator DR Omondi 2/3/2021elishaAinda não há avaliações
- Pt-Case PresentationDocumento19 páginasPt-Case Presentationapi-506024957Ainda não há avaliações
- Caldwell TechniqueDocumento4 páginasCaldwell TechniqueNurul RamadhantyAinda não há avaliações
- List of Books To Read For Dental Pre PG Exams in India DentalDocumento5 páginasList of Books To Read For Dental Pre PG Exams in India Dentalteju patneediAinda não há avaliações
- PRINCIPLES OF CAVITY PREPARATIONDocumento77 páginasPRINCIPLES OF CAVITY PREPARATIONSumanth PhaniAinda não há avaliações
- Caries Detection and Diagnosis Sealants and Management of The Possibly Carious Fissure PDFDocumento7 páginasCaries Detection and Diagnosis Sealants and Management of The Possibly Carious Fissure PDFGen LCAinda não há avaliações
- Misch Seminar Final 6-4-12Documento2 páginasMisch Seminar Final 6-4-12florin013Ainda não há avaliações
- Dwsi Minor Oral SurgDocumento30 páginasDwsi Minor Oral SurgDRRADNANHAinda não há avaliações
- Management of Intricate S-Shaped Root Canals - An Endodontist's ChallengeDocumento4 páginasManagement of Intricate S-Shaped Root Canals - An Endodontist's ChallengeAdvanced Research PublicationsAinda não há avaliações
- Bioclear Posterior KitDocumento32 páginasBioclear Posterior KitSilvio DTAinda não há avaliações
- Eric Whaites Dental Radiology PDFDocumento2 páginasEric Whaites Dental Radiology PDFTiffany0% (2)
- Endovac Whitepaper 1Documento20 páginasEndovac Whitepaper 1Shehla SiddiquiAinda não há avaliações
- Guide To Wisdom TeethDocumento67 páginasGuide To Wisdom TeethSilvio DTAinda não há avaliações
- Guidelines for Surgical Endodontic ProceduresDocumento11 páginasGuidelines for Surgical Endodontic ProceduresgrzeniouAinda não há avaliações
- Topical Fluorides and Decalcification ArDocumento164 páginasTopical Fluorides and Decalcification ArArinaAinda não há avaliações
- Endodontology 1: RootsDocumento44 páginasEndodontology 1: RootsCarlos San Martin100% (1)
- Etiology of Periodontal Diseases - II - Role of Calculus and Local FactorsDocumento33 páginasEtiology of Periodontal Diseases - II - Role of Calculus and Local FactorsHeba S RadaidehAinda não há avaliações
- Existing Restoration - Clinical Status: Secondary Caries Marginal Integrity Biomechanical FormDocumento47 páginasExisting Restoration - Clinical Status: Secondary Caries Marginal Integrity Biomechanical FormDaniel WangAinda não há avaliações
- Vital Therapy in Carious ToothDocumento9 páginasVital Therapy in Carious ToothAsh PeiAinda não há avaliações
- Implants in Clinical Dentistry PDFDocumento274 páginasImplants in Clinical Dentistry PDFCristian AndriescuAinda não há avaliações
- Guidelines BookDocumento16 páginasGuidelines BookAdel ElaroudAinda não há avaliações
- Lecture 5 Laser in Operative DentistryDocumento7 páginasLecture 5 Laser in Operative DentistryDt omarAinda não há avaliações
- Pediatric Dentistry Exam QuestionnaireDocumento2 páginasPediatric Dentistry Exam QuestionnaireVagelis RaftopoulosAinda não há avaliações
- Ameloblastoma Report CaseDocumento6 páginasAmeloblastoma Report CaseYuzketAinda não há avaliações
- Armamentarium FOR Basic Oral Surgery: Deepthi P.R. Intern Dept. of Oral SurgeryDocumento140 páginasArmamentarium FOR Basic Oral Surgery: Deepthi P.R. Intern Dept. of Oral SurgeryGabriela Cocieru MotelicaAinda não há avaliações
- Regressive Changes of TeethDocumento45 páginasRegressive Changes of TeethNader AlaizariAinda não há avaliações
- Expert Third Molar Extractions PDFDocumento2 páginasExpert Third Molar Extractions PDFKate0% (1)
- Pickard's Manual-Tooth Wear (Dragged)Documento8 páginasPickard's Manual-Tooth Wear (Dragged)Adit MehtaAinda não há avaliações
- Wisdom Tooth WisdomDocumento134 páginasWisdom Tooth WisdomPaulo Rabelo Jr.Ainda não há avaliações
- Management of Peri-Implant Mucositis and Peri-Implantitis PDFDocumento19 páginasManagement of Peri-Implant Mucositis and Peri-Implantitis PDFgirl33Ainda não há avaliações
- Milestones in Adhesion - GICDocumento9 páginasMilestones in Adhesion - GICParidhi Garg100% (1)
- Endodontic Failures-A Review: Dr. Sadashiv Daokar, DR - Anita.KalekarDocumento6 páginasEndodontic Failures-A Review: Dr. Sadashiv Daokar, DR - Anita.KalekarGunjan GargAinda não há avaliações
- MagnificationDocumento52 páginasMagnificationSiva KumarAinda não há avaliações
- International Dentists Attend Implantology Week at NYU College of DentistryDocumento1 páginaInternational Dentists Attend Implantology Week at NYU College of DentistryDentalLearningAinda não há avaliações
- The Shortened Dental Arch Concept Awareness and Opinion of Dentists in Australia PDFDocumento8 páginasThe Shortened Dental Arch Concept Awareness and Opinion of Dentists in Australia PDFKarina OjedaAinda não há avaliações
- Esthetic Considerations in Interdental Papilla PDFDocumento11 páginasEsthetic Considerations in Interdental Papilla PDFXavier AltamiranoAinda não há avaliações
- Fixed Clinic Manual 2017Documento74 páginasFixed Clinic Manual 2017Khizer's MusicAinda não há avaliações
- Space MaintainerDocumento2 páginasSpace MaintainerFibrianti SeputriAinda não há avaliações
- Romanian Citizenship With MigrationCentrDocumento9 páginasRomanian Citizenship With MigrationCentrsalman azizAinda não há avaliações
- Jop 2017 160820Documento7 páginasJop 2017 160820salman azizAinda não há avaliações
- Evidence Based Endodontics Literature Database: Home Advanced Search FAQ About UsDocumento2 páginasEvidence Based Endodontics Literature Database: Home Advanced Search FAQ About Ussalman azizAinda não há avaliações
- When To Save or Extract A Tooth in The Esthetic Zone - A Commentary - CDEWorld - Continuing Dental EducationDocumento9 páginasWhen To Save or Extract A Tooth in The Esthetic Zone - A Commentary - CDEWorld - Continuing Dental Educationsalman azizAinda não há avaliações
- 10 Free VPN Tools To Surf Anonymously On AndroidDocumento18 páginas10 Free VPN Tools To Surf Anonymously On Androidsalman azizAinda não há avaliações
- Principles of Retentive Pins Placement in Amalgam Restoration in DentistryDocumento8 páginasPrinciples of Retentive Pins Placement in Amalgam Restoration in Dentistrysalman azizAinda não há avaliações
- An Evidence-Based Concept of Shorter, Narrower Dental ImplantsDocumento7 páginasAn Evidence-Based Concept of Shorter, Narrower Dental Implantssalman azizAinda não há avaliações
- 166370424239990504286662979Documento14 páginas166370424239990504286662979salman azizAinda não há avaliações
- Endodontics Technique for Filling Root CanalsDocumento2 páginasEndodontics Technique for Filling Root Canalssalman azizAinda não há avaliações
- Pulpal and Periapical Diagnostic Terminology and Treatment Considerations - Pocket DentistryDocumento4 páginasPulpal and Periapical Diagnostic Terminology and Treatment Considerations - Pocket Dentistrysalman azizAinda não há avaliações
- Short Implants - A Systematic ReviewDocumento17 páginasShort Implants - A Systematic Reviewsalman azizAinda não há avaliações
- GoatDocumento4 páginasGoatsalman azizAinda não há avaliações
- 3 - Retention of Cores - Pocket DentistryDocumento7 páginas3 - Retention of Cores - Pocket Dentistrysalman azizAinda não há avaliações
- Effect of Saliva On Dental CariesJADADocumento8 páginasEffect of Saliva On Dental CariesJADAsalman azizAinda não há avaliações
- Zirconia in Dental Implantology - A ReviewDocumento13 páginasZirconia in Dental Implantology - A Reviewsalman azizAinda não há avaliações
- SaudiEndodJ52114-2383633 063716Documento6 páginasSaudiEndodJ52114-2383633 063716salman azizAinda não há avaliações
- Scopeofendo RegendoDocumento2 páginasScopeofendo Regendosalman azizAinda não há avaliações
- Local Anesthesia in Dentistry - Use of Local Anesthetics During PregnancyDocumento3 páginasLocal Anesthesia in Dentistry - Use of Local Anesthetics During Pregnancysalman azizAinda não há avaliações
- Endo FlapsDocumento6 páginasEndo FlapshopperpotamusAinda não há avaliações
- JR Et Al-2012-Brazilian Oral ResearchDocumento7 páginasJR Et Al-2012-Brazilian Oral Researchsalman azizAinda não há avaliações
- Minamata Convention On MercuryDocumento30 páginasMinamata Convention On MercuryRia CuaAinda não há avaliações
- Salivaomics PDFDocumento3 páginasSalivaomics PDFsalman azizAinda não há avaliações
- HottoothDocumento75 páginasHottoothsalman azizAinda não há avaliações
- Electronic Apex Locator (Part 1)Documento15 páginasElectronic Apex Locator (Part 1)salman azizAinda não há avaliações
- Endo Overfills Good Bad UglyDocumento5 páginasEndo Overfills Good Bad Uglysalman azizAinda não há avaliações
- Fiber PrefabDocumento6 páginasFiber Prefabsalman azizAinda não há avaliações
- Measures of Disease Frequency PDFDocumento23 páginasMeasures of Disease Frequency PDFsalman azizAinda não há avaliações
- Aus PrescriberDocumento40 páginasAus Prescribersalman azizAinda não há avaliações
- 2 GP Compaction TechniquesDocumento9 páginas2 GP Compaction Techniquessalman azizAinda não há avaliações
- AC Circuit 2 (Three-Phase)Documento2 páginasAC Circuit 2 (Three-Phase)marlon desaculaAinda não há avaliações
- Fischer Carbene Complexes in Organic SynthesisDocumento9 páginasFischer Carbene Complexes in Organic SynthesisNorah AltayyarAinda não há avaliações
- MA 102 Tutorial Sheet No. 2 on Limits and ContinuityDocumento1 páginaMA 102 Tutorial Sheet No. 2 on Limits and ContinuityKanan KumarAinda não há avaliações
- MP Birla Group: Training MatrixDocumento3 páginasMP Birla Group: Training MatrixAprilia kusumaAinda não há avaliações
- Sea Cucumber PDFDocumento171 páginasSea Cucumber PDFRebeccaSulivanAinda não há avaliações
- Anatomy Mckinley PPT Chapter 1Documento65 páginasAnatomy Mckinley PPT Chapter 1Rosa AlcantarAinda não há avaliações
- Heidegger On Destruction - Chung ChinDocumento16 páginasHeidegger On Destruction - Chung ChinAprilo DielovaAinda não há avaliações
- Creative NonfictionDocumento11 páginasCreative NonfictionRubelyn CagapeAinda não há avaliações
- 72 Names of God in HasidimDocumento16 páginas72 Names of God in HasidimFrancesco VinciguerraAinda não há avaliações
- M.E. (Mechanical - Heat Power Engineering) SyllabusDocumento37 páginasM.E. (Mechanical - Heat Power Engineering) SyllabusKapil KotangaleAinda não há avaliações
- Bep Rev.c-New 20 MLD WTP, NathavaliDocumento380 páginasBep Rev.c-New 20 MLD WTP, NathavaliAnonymous 7l8AIyq2Ainda não há avaliações
- Tabel Benkelman Beam Baru - AsisDocumento21 páginasTabel Benkelman Beam Baru - AsisAsisAinda não há avaliações
- Plant Seedling Classification Using CNNDocumento12 páginasPlant Seedling Classification Using CNNYugal Joshi0% (1)
- Explore the Precambrian EraDocumento3 páginasExplore the Precambrian EraArjay CarolinoAinda não há avaliações
- 3 1Documento4 páginas3 1HakanAinda não há avaliações
- Chemistry PropertiesDocumento14 páginasChemistry PropertiesconchoAinda não há avaliações
- EV1116 Manual 146251999-4DDocumento32 páginasEV1116 Manual 146251999-4Danitha ferryAinda não há avaliações
- Djoko The Indonesian Mineral Mining Sector Prospects and ChallengesDocumento42 páginasDjoko The Indonesian Mineral Mining Sector Prospects and ChallengesUmesh ShanmugamAinda não há avaliações
- TOEFL Module 1 - ReadingDocumento65 páginasTOEFL Module 1 - ReadingImam NurviyantoAinda não há avaliações
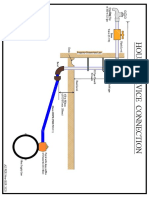
- House Service Connection NEW BSR 2020-1Documento1 páginaHouse Service Connection NEW BSR 2020-1Deshraj BairwaAinda não há avaliações
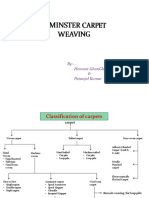
- Axminster CarpetDocumento19 páginasAxminster Carpetrohit sinhaAinda não há avaliações
- IMG - 0092 PSME Code 2012 90Documento1 páginaIMG - 0092 PSME Code 2012 90Bugoy2023Ainda não há avaliações
- CPE PRACTICE TEST 2 READINGDocumento4 páginasCPE PRACTICE TEST 2 READINGHong Anh0% (1)
- Reservoir Engineering Handbook Tarek Ahmed Solution ManualDocumento36 páginasReservoir Engineering Handbook Tarek Ahmed Solution ManualMohamad Hasen japerAinda não há avaliações
- Audit Reveals Optimization Opportunities for Cement Ball Mill SystemDocumento19 páginasAudit Reveals Optimization Opportunities for Cement Ball Mill SystemVijay Bhan100% (2)
- PWC Verbal Past Question and Answer 1Documento130 páginasPWC Verbal Past Question and Answer 1Anton PermanaAinda não há avaliações
- Minicap FTC260, FTC262: Technical InformationDocumento20 páginasMinicap FTC260, FTC262: Technical InformationAmanda PorterAinda não há avaliações
- The Earls Sinful Quest - Lisa CampellDocumento148 páginasThe Earls Sinful Quest - Lisa CampellEirini DiamantopoulouAinda não há avaliações
- The UFO MonthlyDocumento21 páginasThe UFO MonthlySAB78Ainda não há avaliações
- Design of Goods & Services: Tanweer Ascem KharralDocumento10 páginasDesign of Goods & Services: Tanweer Ascem KharralHadeed GulAinda não há avaliações