Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- Strengths and LimitationsDocumento1 páginaStrengths and Limitationsrobby_94Ainda não há avaliações
- The MicroscopeDocumento28 páginasThe Microscoperobby_94Ainda não há avaliações
- The Microscope (ASLI)Documento29 páginasThe Microscope (ASLI)robby_94Ainda não há avaliações
- History of Microscope: Bending Light: The Objective (Bottom) Convex Lens Magnifies and Focuses (Bends)Documento2 páginasHistory of Microscope: Bending Light: The Objective (Bottom) Convex Lens Magnifies and Focuses (Bends)robby_94Ainda não há avaliações
- Sterilizes Food Spores Milk Milk Fruit Juices Cream Soy Milk Yogurt Wine Soups Honey StewsDocumento1 páginaSterilizes Food Spores Milk Milk Fruit Juices Cream Soy Milk Yogurt Wine Soups Honey Stewsrobby_94Ainda não há avaliações
- KDIGO CKD Guideline Manila - KasiskeDocumento66 páginasKDIGO CKD Guideline Manila - Kasiskerobby_94Ainda não há avaliações
- Liver Cirrhosis: Fardah AkilDocumento6 páginasLiver Cirrhosis: Fardah Akilrobby_94Ainda não há avaliações
- ReferatDocumento31 páginasReferatrobby_94Ainda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Idioms and PharsesDocumento0 páginaIdioms and PharsesPratik Ramesh Pappali100% (1)
- City of Atlanta - Structural Checklist: All Items Listed Herein Shall Be Complied With If Applicable To The ProjectDocumento16 páginasCity of Atlanta - Structural Checklist: All Items Listed Herein Shall Be Complied With If Applicable To The ProjectSandip SurAinda não há avaliações
- Starters Flash CardsDocumento28 páginasStarters Flash CardsNara GarridoAinda não há avaliações
- Silly VersesDocumento29 páginasSilly Verseskevin daleAinda não há avaliações
- Ethnomedicinal Plants For Indigestion in Uthiramerur Taluk Kancheepuram District Tamilnadu IndiaDocumento8 páginasEthnomedicinal Plants For Indigestion in Uthiramerur Taluk Kancheepuram District Tamilnadu IndiaGladys DjeugaAinda não há avaliações
- Pamela Johnson Arnold and Nancy Fortson On Behalf of A Minor Vs Hamilton Co. Dept. of EducationDocumento27 páginasPamela Johnson Arnold and Nancy Fortson On Behalf of A Minor Vs Hamilton Co. Dept. of EducationDan LehrAinda não há avaliações
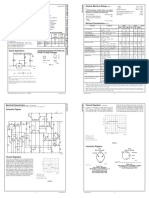
- LM 337Documento4 páginasLM 337matias robertAinda não há avaliações
- Rotary Vane PumpsDocumento7 páginasRotary Vane PumpshebsonbezerraAinda não há avaliações
- Cat 880620 R11Documento60 páginasCat 880620 R11pawelprusAinda não há avaliações
- Boli Vertebro MedulareDocumento12 páginasBoli Vertebro MedulareHalit DianaAinda não há avaliações
- BDC 6566Documento6 páginasBDC 6566jack.simpson.changAinda não há avaliações
- Chemrite SP 200Documento3 páginasChemrite SP 200ghazanfarAinda não há avaliações
- Little Ann and Other Poems by Ann Taylor and Jane TaylorDocumento41 páginasLittle Ann and Other Poems by Ann Taylor and Jane Tayloralexa alexaAinda não há avaliações
- The Coca-Cola Company - Wikipedia, The Free EncyclopediaDocumento11 páginasThe Coca-Cola Company - Wikipedia, The Free EncyclopediaAbhishek ThakurAinda não há avaliações
- 1Manuscript-BSN-3y2-1A-CEDILLO-222 11111Documento32 páginas1Manuscript-BSN-3y2-1A-CEDILLO-222 11111SHARMAINE ANNE POLICIOSAinda não há avaliações
- Evidence-Based Strength & HypertrophyDocumento6 páginasEvidence-Based Strength & HypertrophyAnže BenkoAinda não há avaliações
- Jurnal Gerd PDFDocumento6 páginasJurnal Gerd PDFdilaAinda não há avaliações
- Topic 7: Respiration, Muscles and The Internal Environment Chapter 7B: Muscles, Movement and The HeartDocumento4 páginasTopic 7: Respiration, Muscles and The Internal Environment Chapter 7B: Muscles, Movement and The HeartsalmaAinda não há avaliações
- Top 6 Beginner Work Out MistakesDocumento4 páginasTop 6 Beginner Work Out MistakesMARYAM GULAinda não há avaliações
- Plastic Omnium 2015 RegistrationDocumento208 páginasPlastic Omnium 2015 Registrationgsravan_23Ainda não há avaliações
- Planificare Săptămânală - Clasa A II-a (Fairyland 2)Documento6 páginasPlanificare Săptămânală - Clasa A II-a (Fairyland 2)Oxy Oxy100% (1)
- Dynamic Stretching - Stability - Strength.570239Documento2 páginasDynamic Stretching - Stability - Strength.570239Sylvia GraceAinda não há avaliações
- OM Mannual FOsDocumento38 páginasOM Mannual FOsAbdulmuqtadetr AhmadiAinda não há avaliações
- Ce Mark - Application FormDocumento3 páginasCe Mark - Application Formrajivsinghal90Ainda não há avaliações
- GeoSS Event Seminar 12 July 2012 - SlidesDocumento15 páginasGeoSS Event Seminar 12 July 2012 - SlidesNurmanda RamadhaniAinda não há avaliações
- 03 Secondary School Student's Academic Performance Self Esteem and School Environment An Empirical Assessment From NigeriaDocumento10 páginas03 Secondary School Student's Academic Performance Self Esteem and School Environment An Empirical Assessment From NigeriaKienstel GigantoAinda não há avaliações
- Factors That Contribute To Successful BakingDocumento8 páginasFactors That Contribute To Successful BakingErrol San Juan100% (1)
- Geometry of N-BenzylideneanilineDocumento5 páginasGeometry of N-BenzylideneanilineTheo DianiarikaAinda não há avaliações
- Mon AnhDocumento7 páginasMon AnhDavid NguyenAinda não há avaliações