Você também pode gostar
- Pericarditis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandPericarditis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNota: 5 de 5 estrelas5/5 (3)
- Anticoagulant, Fibrinolytic, and Antiplatelet DrugsDocumento22 páginasAnticoagulant, Fibrinolytic, and Antiplatelet DrugsVera Waty100% (1)
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsNo EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsAinda não há avaliações
- Coagulants and Anti CoagulantsDocumento22 páginasCoagulants and Anti Coagulantsdhainey100% (2)
- A Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsNo EverandA Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsAinda não há avaliações
- Renal Excretion of DrugsDocumento3 páginasRenal Excretion of DrugsGerardLum100% (3)
- Updated Antibiotic Chart - 2016 PDFDocumento2 páginasUpdated Antibiotic Chart - 2016 PDFmugenzi eric100% (1)
- Cholinergics and Cholinergic BlockersDocumento5 páginasCholinergics and Cholinergic Blockersapi-3739910100% (3)
- Anticoagulation Care GuideDocumento13 páginasAnticoagulation Care GuideSadiah Hasyim AlweiniAinda não há avaliações
- Chad Pressors HandoutDocumento12 páginasChad Pressors HandoutquelspectacleAinda não há avaliações
- Thrombolytics, Anticoags, Antiplatelets PDFDocumento21 páginasThrombolytics, Anticoags, Antiplatelets PDFrachelkdoAinda não há avaliações
- Cardiovascular Drug IntroductionDocumento3 páginasCardiovascular Drug IntroductionSamah Khan100% (1)
- Stages of ShockDocumento13 páginasStages of ShockA. P.Ainda não há avaliações
- Common Cardiac MedicationsDocumento1 páginaCommon Cardiac MedicationsPaige HardekopfAinda não há avaliações
- Cardiogenic ShockDocumento2 páginasCardiogenic ShockChristine QuironaAinda não há avaliações
- Blood Conservation StrategiesDocumento31 páginasBlood Conservation Strategiesthalida24100% (1)
- Cardiac Emergencies Cne DelhiDocumento109 páginasCardiac Emergencies Cne DelhiManisha Thakur100% (1)
- Preload and AfterloadDocumento4 páginasPreload and AfterloadNeranga SamaratungeAinda não há avaliações
- Ch-13 Drugs Used in Heart FailureDocumento49 páginasCh-13 Drugs Used in Heart FailureShabrin SadikhAinda não há avaliações
- Topic Discussion Heart Failure MedicationsDocumento7 páginasTopic Discussion Heart Failure Medicationsapi-385309917Ainda não há avaliações
- Adrenergic Drugs 20.07.018 PDFDocumento59 páginasAdrenergic Drugs 20.07.018 PDFHitesh karnAinda não há avaliações
- Antihypertensive DrugsDocumento29 páginasAntihypertensive Drugsmailforrandomuse100% (1)
- Pathogenesis of Micro and Macrovascular Complications of DiabetesDocumento4 páginasPathogenesis of Micro and Macrovascular Complications of DiabetesFrancesca LiAinda não há avaliações
- Approximate Equivalents:: 0.100 Gmn. 1.00 GMDocumento8 páginasApproximate Equivalents:: 0.100 Gmn. 1.00 GMakane ryuAinda não há avaliações
- Cardiovascular Pharmacology: - Hypertension - Angina Pectoris - Cardiac Arrhythmias - Heart FailureDocumento31 páginasCardiovascular Pharmacology: - Hypertension - Angina Pectoris - Cardiac Arrhythmias - Heart Failurelynch775100% (2)
- Cardiac ArrhythmiasDocumento9 páginasCardiac ArrhythmiasRemelou Garchitorena AlfelorAinda não há avaliações
- Hypertensive EmergenciesDocumento49 páginasHypertensive EmergenciesSafa Abdualrahaman Ali HamadAinda não há avaliações
- Med Geeks Clinical Lab GuideDocumento17 páginasMed Geeks Clinical Lab GuideHuy Hoang100% (1)
- ECG InterpretationDocumento95 páginasECG InterpretationShiela Mae Lopez100% (10)
- Categorization of Rabies Exposure HypertensionDocumento2 páginasCategorization of Rabies Exposure HypertensionNikki ValerioAinda não há avaliações
- Portal HypertensionDocumento103 páginasPortal Hypertensionsolysan50% (2)
- Inotropes and VasopressorsDocumento56 páginasInotropes and VasopressorsMuhammad Ali Yousuf100% (6)
- BurnsDocumento80 páginasBurnsmarAinda não há avaliações
- Antihypertensive AgentsDocumento2 páginasAntihypertensive Agentskryscae nacarAinda não há avaliações
- Drugs For Heart Failure: Drugs Catego Ry Drug Function Adverse Effect NoteDocumento2 páginasDrugs For Heart Failure: Drugs Catego Ry Drug Function Adverse Effect NoteyukariAinda não há avaliações
- Immunosuppressant Drugs Drug Name Class Function Method/Receptor UseDocumento3 páginasImmunosuppressant Drugs Drug Name Class Function Method/Receptor UseKristin DouglasAinda não há avaliações
- Sepsis and Septic ShockDocumento4 páginasSepsis and Septic Shocksarguss14100% (4)
- Pericarditis 65 SlidesDocumento65 páginasPericarditis 65 SlidesAtifBhoreAinda não há avaliações
- Advanced ECG Interpretation: Rebecca Sevigny BSN, RN, CCRNDocumento76 páginasAdvanced ECG Interpretation: Rebecca Sevigny BSN, RN, CCRNI Putu SastrawanAinda não há avaliações
- DyslipidemiaDocumento44 páginasDyslipidemiaenri100% (1)
- Dyspnea and HypoxiaDocumento9 páginasDyspnea and Hypoxiadtimtiman100% (3)
- Snake Bite ToxiconDocumento14 páginasSnake Bite ToxiconAETCM Emergency medicine100% (1)
- Congestive Heart FailureDocumento17 páginasCongestive Heart FailureLyana StarkAinda não há avaliações
- Anti Hypertensive Drugs - ACE InhibitorDocumento16 páginasAnti Hypertensive Drugs - ACE InhibitorApurba Sarker Apu100% (1)
- Assessment of Right Ventricular FunctionDocumento41 páginasAssessment of Right Ventricular FunctionAditya MadhavpeddiAinda não há avaliações
- Cardiovascular Assessment Pocket Reference Card PDFDocumento8 páginasCardiovascular Assessment Pocket Reference Card PDFerikaAinda não há avaliações
- CCPC15 Acute Cardiac Care Workbook PDFDocumento42 páginasCCPC15 Acute Cardiac Care Workbook PDFMina Samir BesharaAinda não há avaliações
- Fluid ResuscitationDocumento23 páginasFluid ResuscitationDunstan Abel SambatangAinda não há avaliações
- GI MnemonicsDocumento14 páginasGI Mnemonicsjonnyahn100% (1)
- 1 - Fluid and Electrolytes (Schwartz Based)Documento52 páginas1 - Fluid and Electrolytes (Schwartz Based)Alexandra RebosuraAinda não há avaliações
- Liver Lab Essentials Liver Lab Essentials: Amer Wahed, MDDocumento53 páginasLiver Lab Essentials Liver Lab Essentials: Amer Wahed, MDAbdulrahman M AlharbiAinda não há avaliações
- Approach To Trauma PatientDocumento49 páginasApproach To Trauma PatientHadinur Jufri100% (1)
- Blood Gas AnalysisDocumento3 páginasBlood Gas AnalysisChameera Bandara100% (2)
- Lecture 4: Hypovolemic ShockDocumento20 páginasLecture 4: Hypovolemic Shockj.doe.hex_87Ainda não há avaliações
- CHAPTER 27 - Heart Failure With A Preserved Ejection FractionDocumento15 páginasCHAPTER 27 - Heart Failure With A Preserved Ejection FractionReda SoAinda não há avaliações
- Ecg Interpretation: Intervals and ComplexesDocumento7 páginasEcg Interpretation: Intervals and ComplexesBobet ReñaAinda não há avaliações
- ECG Master Class-2Documento138 páginasECG Master Class-2Shohag ID Center100% (1)
- Ace Inhibitors MnemonicDocumento1 páginaAce Inhibitors MnemonicGirish Waru0% (2)
- Resuscitation Pharmacology: Dr. Beny Hartono, SPJP, FihaDocumento44 páginasResuscitation Pharmacology: Dr. Beny Hartono, SPJP, FihaAna AgustinaAinda não há avaliações
- Valvular Heart Disease: Aortic Stenosis Aortic Regurgitation Mitral Stenosis Mitral Regurgitation Common EtiologiesDocumento2 páginasValvular Heart Disease: Aortic Stenosis Aortic Regurgitation Mitral Stenosis Mitral Regurgitation Common Etiologiesanisal489Ainda não há avaliações
- Jfas Original ResearchDocumento12 páginasJfas Original ResearchTyler Lawrence CoyeAinda não há avaliações
- Operative Techniques in Foot and Ankle Surgery - (Axial Screw Technique For Midfoot Arthrodesis in Charcot Foot Deformit... )Documento7 páginasOperative Techniques in Foot and Ankle Surgery - (Axial Screw Technique For Midfoot Arthrodesis in Charcot Foot Deformit... )Tyler Lawrence CoyeAinda não há avaliações
- Treatment of Lisfranc Fracture-Dislocations With PDocumento8 páginasTreatment of Lisfranc Fracture-Dislocations With PTyler Lawrence CoyeAinda não há avaliações
- Luke Vetti - NBPME Part 1 - LEA - Anterior Hip + Gluteal Muscles 1Documento3 páginasLuke Vetti - NBPME Part 1 - LEA - Anterior Hip + Gluteal Muscles 1Tyler Lawrence CoyeAinda não há avaliações
- Dfa 6 29629Documento12 páginasDfa 6 29629Tyler Lawrence CoyeAinda não há avaliações
- Meta-Analysis of Diagnostic Accuracy With Mada: Philipp Doebler Heinz HollingDocumento21 páginasMeta-Analysis of Diagnostic Accuracy With Mada: Philipp Doebler Heinz HollingTyler Lawrence CoyeAinda não há avaliações
- READMEDocumento1 páginaREADMETyler Lawrence CoyeAinda não há avaliações
- Podiatry Institute ManualDocumento301 páginasPodiatry Institute ManualTyler Lawrence Coye100% (2)
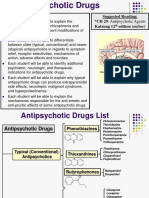
- AntipsychoticsDocumento29 páginasAntipsychoticsTyler Lawrence Coye100% (5)
- Trauma Workshop 1Documento10 páginasTrauma Workshop 1Tyler Lawrence CoyeAinda não há avaliações
- Penn Presby Residency Manual PodiatryDocumento400 páginasPenn Presby Residency Manual PodiatryTyler Lawrence Coye100% (1)
- Trauma Manual (Podiatry)Documento403 páginasTrauma Manual (Podiatry)QuantumjanitorAinda não há avaliações
- Ankle Instability 2017-2018Documento44 páginasAnkle Instability 2017-2018Tyler Lawrence CoyeAinda não há avaliações
- 16 Principles of Ankle and Foot CTDocumento48 páginas16 Principles of Ankle and Foot CTTyler Lawrence CoyeAinda não há avaliações
- Lecture-12-2 22 17Documento7 páginasLecture-12-2 22 17Tyler Lawrence CoyeAinda não há avaliações
- Lecture 3 Capsule Tendon Balance ProceduresDocumento19 páginasLecture 3 Capsule Tendon Balance ProceduresTyler Lawrence CoyeAinda não há avaliações
- Anti EpilepticsDocumento46 páginasAnti EpilepticsTyler Lawrence CoyeAinda não há avaliações
- The Principles of Antibiotic Therapy: S. Aureus Streptococcus PneumoniaeDocumento16 páginasThe Principles of Antibiotic Therapy: S. Aureus Streptococcus PneumoniaeDianne Chua100% (7)
- Goljan Step 1 HY 36 Pages Notes PDFDocumento36 páginasGoljan Step 1 HY 36 Pages Notes PDFTyler Lawrence CoyeAinda não há avaliações
- Wound and Skin Ulcer Management Care Guide PDFDocumento21 páginasWound and Skin Ulcer Management Care Guide PDFAdriel Chandra AngAinda não há avaliações
- 09 Vascular TraumaDocumento36 páginas09 Vascular TraumaTyler Lawrence CoyeAinda não há avaliações
- Respratory Drugs I-IIDocumento10 páginasRespratory Drugs I-IITyler Lawrence CoyeAinda não há avaliações
- Venous DiseaseDocumento19 páginasVenous DiseaseTyler Lawrence CoyeAinda não há avaliações
- Crozer Manual - Second Edition PDFDocumento219 páginasCrozer Manual - Second Edition PDFTyler Lawrence CoyeAinda não há avaliações
- Chapter 8 - Head and Neck 2015Documento72 páginasChapter 8 - Head and Neck 2015Tyler Lawrence CoyeAinda não há avaliações
- Mit PDFDocumento106 páginasMit PDFTyler Lawrence CoyeAinda não há avaliações
- The Ohio Book - LEA DiagramsDocumento168 páginasThe Ohio Book - LEA DiagramsTyler Lawrence Coye100% (2)
- Drugs Class Mechanism: Guaifenesin (OTC)Documento10 páginasDrugs Class Mechanism: Guaifenesin (OTC)Tyler Lawrence CoyeAinda não há avaliações
- Anatomy RecallDocumento337 páginasAnatomy RecallTyler Lawrence Coye100% (2)
- Blood Coagulation SeminarDocumento115 páginasBlood Coagulation SeminarmeghaAinda não há avaliações
- A Brief History of HemophiliaDocumento127 páginasA Brief History of HemophiliaApurba SahaAinda não há avaliações
- DR Ip (Perbedaan Profil Perdarahan Pemberian Antiplatelet Pada Pasien Stroke Iskemik - Mukernas Perdossi Yogyakarta 27-30 Juli 2017Documento15 páginasDR Ip (Perbedaan Profil Perdarahan Pemberian Antiplatelet Pada Pasien Stroke Iskemik - Mukernas Perdossi Yogyakarta 27-30 Juli 2017fajarrudy qimindraAinda não há avaliações
- 1 s2.0 S0140673603134058 MainDocumento9 páginas1 s2.0 S0140673603134058 MainΚωνσταντίνος ΤσίπηςAinda não há avaliações
- Coagulation Cascade: Difference Between Intrinsic and Extrinsic PathwayDocumento10 páginasCoagulation Cascade: Difference Between Intrinsic and Extrinsic Pathwayroshmae100% (1)
- Heme Quiz 1-3Documento14 páginasHeme Quiz 1-3Søren KierkegaardAinda não há avaliações
- DivitiDocumento36 páginasDivitiMarLeniRNAinda não há avaliações
- DOAC - Review Article Direct Oral AnticoagulantsDocumento12 páginasDOAC - Review Article Direct Oral AnticoagulantsborstAinda não há avaliações
- Chap4 Hemodynamics F2Documento12 páginasChap4 Hemodynamics F2Twinkle Salonga100% (3)
- HaemophiliaDocumento15 páginasHaemophiliaSanmuga VimalanathanAinda não há avaliações
- Blood Pharmacology by Dr. Mayur Sayta M 910444Documento21 páginasBlood Pharmacology by Dr. Mayur Sayta M 910444funzz100% (1)
- A Cell-Based Model of Coagulation and The Role of Factor VIIa - Blood Review 2003Documento5 páginasA Cell-Based Model of Coagulation and The Role of Factor VIIa - Blood Review 2003Oscar Echeverría OrellanaAinda não há avaliações
- Andexxa Formulary KitDocumento32 páginasAndexxa Formulary KitAlbert ChangAinda não há avaliações
- Sysmex HemostasisDocumento11 páginasSysmex HemostasisElyza L. de GuzmanAinda não há avaliações
- MK Hemodynamics PathologyDocumento27 páginasMK Hemodynamics PathologyMoses Jr Kazevu100% (1)
- Lecture On Hemostasis by Dr. RoomiDocumento43 páginasLecture On Hemostasis by Dr. RoomiMudassar Roomi100% (1)
- Hemostatic and Thrombotic Considerations in The Diagnosis and ManagementDocumento12 páginasHemostatic and Thrombotic Considerations in The Diagnosis and Managementender izaguirreAinda não há avaliações
- Changes Include Addition of Nattokinase As First Line Therapy and Reordering of First-And Second-Line TherapiesDocumento60 páginasChanges Include Addition of Nattokinase As First Line Therapy and Reordering of First-And Second-Line TherapiesJoshua VanhieAinda não há avaliações
- Summary of Product CharacteristicsDocumento24 páginasSummary of Product Characteristicsddandan_2Ainda não há avaliações
- Hemoststic AgentsDocumento17 páginasHemoststic AgentsJoseph John K PothanikatAinda não há avaliações
- Bleeding Disorders: Dairion Gatot, Soegiarto Gani, Savita HandayaniDocumento50 páginasBleeding Disorders: Dairion Gatot, Soegiarto Gani, Savita HandayaniririsAinda não há avaliações
- @MedicalBooksStoreS 2017 Acute IschemicDocumento273 páginas@MedicalBooksStoreS 2017 Acute IschemicAditya Perdana Dharma Wiguna100% (1)
- HemophiliaDocumento60 páginasHemophiliavibhurocksAinda não há avaliações
- CV Disease Drug StudyDocumento11 páginasCV Disease Drug StudyMaria Francheska OsiAinda não há avaliações
- Blood Clotting ChartDocumento1 páginaBlood Clotting ChartBianca SimionescuAinda não há avaliações
- Jurnal Penjamu FixDocumento3 páginasJurnal Penjamu FixUssie Fitrii FauziiahAinda não há avaliações
- 2.7.2. Microbiological Assay of AntibioticsDocumento7 páginas2.7.2. Microbiological Assay of AntibioticsAshen NirodyaAinda não há avaliações
- Faal Hemostasis: Oleh: Dr. Diah Hermayanti, SPPKDocumento46 páginasFaal Hemostasis: Oleh: Dr. Diah Hermayanti, SPPKGranitaAinda não há avaliações
- JJ Notes PhysiologyDocumento192 páginasJJ Notes PhysiologyTanish Patil roll no 50100% (2)