Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Doctor High Yield Obgyn - Not AnnotatedDocumento34 páginasDoctor High Yield Obgyn - Not AnnotatedEmanuella Gomez100% (2)
- Hypertensionin PregnancyDocumento100 páginasHypertensionin Pregnancyricky hutagalungAinda não há avaliações
- Hysteroscopic Limitations PDFDocumento59 páginasHysteroscopic Limitations PDFV R100% (1)
- Nursing Care of A Family During Labor and BirthDocumento19 páginasNursing Care of A Family During Labor and BirthPbAinda não há avaliações
- Combined Orals APGODocumento52 páginasCombined Orals APGOEmilee Tu0% (1)
- Impaired Lactation Review of Delayed Lactogenesis and Insufficient LactationDocumento10 páginasImpaired Lactation Review of Delayed Lactogenesis and Insufficient LactationRob BordenAinda não há avaliações
- Abnormalities of Placenta and CordDocumento47 páginasAbnormalities of Placenta and CordShrooti Shah75% (4)
- MANAGEMENT OF 3rd AND 4th STAGEDocumento18 páginasMANAGEMENT OF 3rd AND 4th STAGENidhi Sharma100% (1)
- Association Between MRNA Expression of Aromatase 1Documento8 páginasAssociation Between MRNA Expression of Aromatase 1Nenny Yoanitha DjalaAinda não há avaliações
- Estimated Fetal Weight Formula GuideDocumento5 páginasEstimated Fetal Weight Formula GuideNenny Yoanitha Djala100% (1)
- Palliative Care - Modul NennyDocumento31 páginasPalliative Care - Modul NennyNenny Yoanitha DjalaAinda não há avaliações
- Reichman 2014Documento5 páginasReichman 2014Nenny Yoanitha DjalaAinda não há avaliações
- Program Kerja Gugus Kendali Mutu SMF Obstetri dan Ginekologi 2017-2018Documento1 páginaProgram Kerja Gugus Kendali Mutu SMF Obstetri dan Ginekologi 2017-2018Nenny Yoanitha DjalaAinda não há avaliações
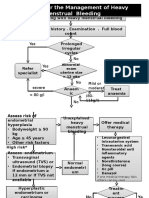
- Algorithm For The Management of Heavy Menstrual BleedingDocumento2 páginasAlgorithm For The Management of Heavy Menstrual BleedingNenny Yoanitha DjalaAinda não há avaliações
- Night Shift Duty 11 FEBRUARIDocumento2 páginasNight Shift Duty 11 FEBRUARINenny Yoanitha DjalaAinda não há avaliações
- AJOG 2008 - Amoxicillin Pharmacokinetics in Pregnant WomenDocumento6 páginasAJOG 2008 - Amoxicillin Pharmacokinetics in Pregnant WomenNenny Yoanitha DjalaAinda não há avaliações
- Final Data 2011 PDFDocumento90 páginasFinal Data 2011 PDFNenny Yoanitha DjalaAinda não há avaliações
- Termination Pregnancy Report 18 May 2010Documento45 páginasTermination Pregnancy Report 18 May 2010Nenny Yoanitha DjalaAinda não há avaliações
- Algorithm For The Management of Heavy Menstrual BleedingDocumento2 páginasAlgorithm For The Management of Heavy Menstrual BleedingNenny Yoanitha DjalaAinda não há avaliações
- En Endometrial Cancer Guide For PatientsDocumento30 páginasEn Endometrial Cancer Guide For PatientsNenny Yoanitha DjalaAinda não há avaliações
- Medical Eligibility Criteria For Contraceptive Use Fifth Edition 2015Documento14 páginasMedical Eligibility Criteria For Contraceptive Use Fifth Edition 2015agustinasntAinda não há avaliações
- Algorithm For The Management of Heavy Menstrual BleedingDocumento2 páginasAlgorithm For The Management of Heavy Menstrual BleedingNenny Yoanitha DjalaAinda não há avaliações
- Strategi Bisnis KorporasiDocumento41 páginasStrategi Bisnis KorporasiAliMu'minHarahapAinda não há avaliações
- Anatomical Causes Bad Obstetric HistoryDocumento3 páginasAnatomical Causes Bad Obstetric Historykyle31Ainda não há avaliações
- Reichman 2014Documento5 páginasReichman 2014Nenny Yoanitha DjalaAinda não há avaliações
- Forceps Review in Modern Obstetric PracticeDocumento5 páginasForceps Review in Modern Obstetric PracticeNenny Yoanitha DjalaAinda não há avaliações
- Fetal and Maternal Effects of Forceps and VacuumDocumento4 páginasFetal and Maternal Effects of Forceps and VacuumNenny Yoanitha DjalaAinda não há avaliações
- Genetic Study of TORCH Infections in Women With BOH PDFDocumento6 páginasGenetic Study of TORCH Infections in Women With BOH PDFNenny Yoanitha DjalaAinda não há avaliações
- Trali Dari Ats JournalDocumento2 páginasTrali Dari Ats JournalNenny Yoanitha DjalaAinda não há avaliações
- Reichman 2014Documento5 páginasReichman 2014Nenny Yoanitha DjalaAinda não há avaliações
- Forceps ExtractionDocumento49 páginasForceps ExtractionNenny Yoanitha DjalaAinda não há avaliações
- How To Explore After Forceps ExtractionDocumento7 páginasHow To Explore After Forceps ExtractionNenny Yoanitha DjalaAinda não há avaliações
- Obstetrical Forceps - History Mystery and MoralityDocumento16 páginasObstetrical Forceps - History Mystery and MoralityNenny Yoanitha DjalaAinda não há avaliações
- Successful Pregnancy OutcomeDocumento6 páginasSuccessful Pregnancy OutcomeNenny Yoanitha DjalaAinda não há avaliações
- Cytomegalovirus Infection in Patients With Active InflammatoryDocumento7 páginasCytomegalovirus Infection in Patients With Active InflammatoryNenny Yoanitha DjalaAinda não há avaliações
- ANTEPARTUMDocumento4 páginasANTEPARTUMcoosa liquorsAinda não há avaliações
- 2008, Vol.92, Issues 5, Women's HealthDocumento312 páginas2008, Vol.92, Issues 5, Women's HealthHussain OudahAinda não há avaliações
- Assessment of Breast and Lymphatic SystemDocumento4 páginasAssessment of Breast and Lymphatic Systemclyde i amAinda não há avaliações
- Family Case Study 1Documento12 páginasFamily Case Study 1Mark Anthony Torcino AbianAinda não há avaliações
- 1 RESU Tally Sheet For Pregnant Women 1 REPORTDocumento6 páginas1 RESU Tally Sheet For Pregnant Women 1 REPORTJoe Pete TiuAinda não há avaliações
- Obstetric Anal Sphincter Injury-FoudaDocumento36 páginasObstetric Anal Sphincter Injury-FoudaMade DarmayasaAinda não há avaliações
- Menstrual CycleDocumento16 páginasMenstrual CycleDikpal BikramAinda não há avaliações
- Urinary Retention PostpartumDocumento5 páginasUrinary Retention PostpartumpaswordnyalupaAinda não há avaliações
- Anatomy & Physiology (Chapter 19 - Reproductive System)Documento30 páginasAnatomy & Physiology (Chapter 19 - Reproductive System)Eduardo Niepes Jr.Ainda não há avaliações
- CAT 1 CMT 05207 REPRODUCTIVE AND CHILD HEALTH NameDocumento9 páginasCAT 1 CMT 05207 REPRODUCTIVE AND CHILD HEALTH NamenanjegovictoriaAinda não há avaliações
- Oogenesis and The Ovarian Cycle: Angelbert R. Bacongco Justin Rhea M. BandiolaDocumento19 páginasOogenesis and The Ovarian Cycle: Angelbert R. Bacongco Justin Rhea M. BandiolaJustin Rhea BandiolaAinda não há avaliações
- Preterm Labour: Muhammad Hanif Final Year MBBSDocumento32 páginasPreterm Labour: Muhammad Hanif Final Year MBBSArslan HassanAinda não há avaliações
- Pathology ofDocumento114 páginasPathology ofRahul Audenesen BratAinda não há avaliações
- Gynecology Notes Legal Issues and EthicsDocumento19 páginasGynecology Notes Legal Issues and EthicsUsm LeeAinda não há avaliações
- HISTOLOGY-NOTES-by-Red ReproductiveDocumento6 páginasHISTOLOGY-NOTES-by-Red ReproductiveEdzeal Bruan JrAinda não há avaliações
- Maternity MOH 333 PDFDocumento4 páginasMaternity MOH 333 PDFMajivaAinda não há avaliações
- Misoprostol PDFDocumento5 páginasMisoprostol PDFEduardAinda não há avaliações
- Ectopic Molar Pregnancy A Case ReportDocumento4 páginasEctopic Molar Pregnancy A Case ReportInternational Journal of Innovative Science and Research Technology100% (1)
- Sri Lanka Women's ManifestoDocumento17 páginasSri Lanka Women's ManifestoSocial Scientists' AssociationAinda não há avaliações
- Form EFBDDocumento5 páginasForm EFBDjooner45Ainda não há avaliações
- GonoraeDocumento16 páginasGonoraeOkta KendaAinda não há avaliações
- Hatfield PPT CH 15Documento53 páginasHatfield PPT CH 15HannaAinda não há avaliações
- MCQ sample questions on mechanisms of labour and pregnancy complicationsDocumento11 páginasMCQ sample questions on mechanisms of labour and pregnancy complicationsMuhammad Bilal100% (2)