Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- ACOG Practice Bulletin: Gestational Hypertension and Preeclampsia 2019.Documento25 páginasACOG Practice Bulletin: Gestational Hypertension and Preeclampsia 2019.Jean Paúl LópezAinda não há avaliações
- Abortion EssayDocumento10 páginasAbortion EssayRamizAinda não há avaliações
- Pathogenesis of Preterm LaborDocumento14 páginasPathogenesis of Preterm LaborAgung Sunarko PutraAinda não há avaliações
- Absent End-Diastolic Velocity in The Umbilical Artery and Its Clinical SignificanceDocumento12 páginasAbsent End-Diastolic Velocity in The Umbilical Artery and Its Clinical Significancejakob_saleanAinda não há avaliações
- Delivery Room E-Portfolio: Bartolaba, Lyca RDocumento17 páginasDelivery Room E-Portfolio: Bartolaba, Lyca RLRBAinda não há avaliações
- Pregnancy Simulation Scenario StudentDocumento3 páginasPregnancy Simulation Scenario StudentmarieAinda não há avaliações
- Hypoxic Ischemic EncephalopathyDocumento7 páginasHypoxic Ischemic EncephalopathyJennesse May Guiao IbayAinda não há avaliações
- Drug Therapy Across The LifespanDocumento34 páginasDrug Therapy Across The LifespanJSeasharkAinda não há avaliações
- Sheila C. Woodward. Fetal, Neonatal and Early Infant Experiences of Maternal Singing.Documento29 páginasSheila C. Woodward. Fetal, Neonatal and Early Infant Experiences of Maternal Singing.Юрий Семёнов100% (1)
- Drug Use During Pregnancy and LactationDocumento93 páginasDrug Use During Pregnancy and Lactation2012100% (2)
- MCN Ethical and Social Issues in Prenatal NursingDocumento26 páginasMCN Ethical and Social Issues in Prenatal NursingLhara Vhaneza CuetoAinda não há avaliações
- Obg Prenatal Period Golden Points: Nursing CrashDocumento9 páginasObg Prenatal Period Golden Points: Nursing CrashOmprakash SainiAinda não há avaliações
- MCN Finals NotesDocumento495 páginasMCN Finals NotesLeigh JiandAinda não há avaliações
- Notes On Maternal & Child Care (Pregnancy)Documento3 páginasNotes On Maternal & Child Care (Pregnancy)Oink TopusAinda não há avaliações
- REPRODocumento48 páginasREPROARVIND KUMAR YADAVAinda não há avaliações
- ISUOG Practice Guidelines Updated Performance CompressedDocumento17 páginasISUOG Practice Guidelines Updated Performance CompressedSaranya BalamuruganAinda não há avaliações
- Melody Doria - Chapter 20 ActivityDocumento3 páginasMelody Doria - Chapter 20 ActivityMelody MirandaAinda não há avaliações
- Lydia E Hall's Theory (Nov 06)Documento42 páginasLydia E Hall's Theory (Nov 06)soniya naik100% (2)
- Cognizant Previous Year Papers and Questions: (Green Marked Option Denotes The Correct OptionnDocumento316 páginasCognizant Previous Year Papers and Questions: (Green Marked Option Denotes The Correct OptionnHanuman Sai MajetiAinda não há avaliações
- Indications Contraindications Warnings PrecautionsDocumento3 páginasIndications Contraindications Warnings PrecautionsMelvin ValdezAinda não há avaliações
- The Thrifty Psychiatric PhenotypeDocumento3 páginasThe Thrifty Psychiatric Phenotypeeduardobar2000Ainda não há avaliações
- Charateristics of NewbornDocumento3 páginasCharateristics of NewbornRagupathyRamanjuluAinda não há avaliações
- Curs Pediatrie ENG 2013Documento362 páginasCurs Pediatrie ENG 2013cubixmuresAinda não há avaliações
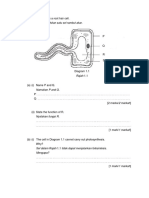
- Rajah 1.1 Menunjukkan Satu Sel Rambut AkarDocumento29 páginasRajah 1.1 Menunjukkan Satu Sel Rambut AkarAzfar SyahmiAinda não há avaliações
- Maternity Nursing An Introductory Text 11th Edition Leifer Test BankDocumento25 páginasMaternity Nursing An Introductory Text 11th Edition Leifer Test BankJenniferNicholsonqknj100% (63)
- Early and Late Preeclamsia Are Characterized by High Cardiac Output, But in The Presence of Fetal Growth Restriction, Cardiac Output Is Low Insights From A Prospective Study PDFDocumento12 páginasEarly and Late Preeclamsia Are Characterized by High Cardiac Output, But in The Presence of Fetal Growth Restriction, Cardiac Output Is Low Insights From A Prospective Study PDFJustiawan NazwanAinda não há avaliações
- Best Practice & Research Clinical Obstetrics and GynaecologyDocumento13 páginasBest Practice & Research Clinical Obstetrics and GynaecologyRodrigoEscobedoAinda não há avaliações
- 2021 July HighlightedDocumento76 páginas2021 July HighlightedAu Cassie100% (5)
- Post Term PregnancyDocumento35 páginasPost Term PregnancyNishaThakuri100% (2)
- Final Why Abortion Should Be Legal.........Documento15 páginasFinal Why Abortion Should Be Legal.........haque163Ainda não há avaliações