Você também pode gostar
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
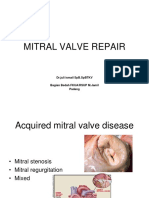
- Mitral Valve Repair: DR - Juli Ismail SPB - SPBTKV Bagian Bedah Fkua/Rsup M.Jamil PadangDocumento22 páginasMitral Valve Repair: DR - Juli Ismail SPB - SPBTKV Bagian Bedah Fkua/Rsup M.Jamil PadangNova SuryatiAinda não há avaliações
- Renal Replacement Therapy in Acute Kidney Injury: Review: Blood Research & Transfusion JournalDocumento4 páginasRenal Replacement Therapy in Acute Kidney Injury: Review: Blood Research & Transfusion JournalNova SuryatiAinda não há avaliações
- Aortic Stenosis: Yerizal Karani MD Cardiology Division Faculty of Medicine Andalas UniversityDocumento29 páginasAortic Stenosis: Yerizal Karani MD Cardiology Division Faculty of Medicine Andalas UniversityNova SuryatiAinda não há avaliações
- Randomized Clinical Trial of Antibiotic Therapy Versus Appendicectomy As Primary Treatment of Acute Appendicitis in Unselected PatientsDocumento9 páginasRandomized Clinical Trial of Antibiotic Therapy Versus Appendicectomy As Primary Treatment of Acute Appendicitis in Unselected PatientsNova SuryatiAinda não há avaliações
- Bacterial Aspect of The Cardiac DiseaseDocumento9 páginasBacterial Aspect of The Cardiac DiseaseNova SuryatiAinda não há avaliações
- Miringitis BulosaDocumento1 páginaMiringitis BulosaNova SuryatiAinda não há avaliações
- Ijcri 1056610201566 AbdelreheemDocumento6 páginasIjcri 1056610201566 AbdelreheemNova SuryatiAinda não há avaliações
- Jurnal VariselaDocumento7 páginasJurnal VariselaNova SuryatiAinda não há avaliações
- Jurnal Varisela ZosterDocumento19 páginasJurnal Varisela ZosterNova SuryatiAinda não há avaliações
- Idiopathic Normal Pressure Hydrocephalus: A Review For General PractitionersDocumento6 páginasIdiopathic Normal Pressure Hydrocephalus: A Review For General PractitionersNova SuryatiAinda não há avaliações
- "Labor and Delivery": Joserizal Serudji Bag/SMF OBGIN FK Unand/RS. M.Djamil PadangDocumento34 páginas"Labor and Delivery": Joserizal Serudji Bag/SMF OBGIN FK Unand/RS. M.Djamil PadangNova SuryatiAinda não há avaliações
- TutorialDocumento13 páginasTutorialNova SuryatiAinda não há avaliações
- Pleno MG 5Documento13 páginasPleno MG 5Nova SuryatiAinda não há avaliações
- Fungsi Mata Dan KulitDocumento4 páginasFungsi Mata Dan KulitNova SuryatiAinda não há avaliações
- Bartholinitis: DiagnosisDocumento11 páginasBartholinitis: DiagnosisNova SuryatiAinda não há avaliações
- Gangguan NutrisiDocumento8 páginasGangguan NutrisiNova SuryatiAinda não há avaliações
- Infeksi Jamur OportunistikDocumento27 páginasInfeksi Jamur OportunistikNova SuryatiAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- PronounsDocumento6 páginasPronounsHải Dương LêAinda não há avaliações
- SAP HR - Legacy System Migration Workbench (LSMW)Documento5 páginasSAP HR - Legacy System Migration Workbench (LSMW)Bharathk KldAinda não há avaliações
- Abc Uae Oil and GasDocumento41 páginasAbc Uae Oil and GasajayAinda não há avaliações
- University Fees Structure (Himalayan Garhwal University) - UttarakhandDocumento1 páginaUniversity Fees Structure (Himalayan Garhwal University) - UttarakhandabhaybaranwalAinda não há avaliações
- MSC ACFN2 RD4 ClassDocumento25 páginasMSC ACFN2 RD4 Classmengistu jiloAinda não há avaliações
- Perturbation MethodsDocumento29 páginasPerturbation Methodsmhdr100% (1)
- Ged 102 Mathematics in The Modern WorldDocumento84 páginasGed 102 Mathematics in The Modern WorldKier FormelozaAinda não há avaliações
- 6 Uec ProgramDocumento21 páginas6 Uec Programsubramanyam62Ainda não há avaliações
- Friday 25 Mar 12:15 AM Friday 25 Mar 5:30 AM: Emirates CGK DXBDocumento3 páginasFriday 25 Mar 12:15 AM Friday 25 Mar 5:30 AM: Emirates CGK DXBDONI ARTAAinda não há avaliações
- BSDDocumento26 páginasBSDEunnicePanaliganAinda não há avaliações
- Ethiopian Airlines-ResultsDocumento1 páginaEthiopian Airlines-Resultsabdirahmanguray46Ainda não há avaliações
- JCIPDocumento5 páginasJCIPdinesh.nayak.bbsrAinda não há avaliações
- Cpar ReviewerDocumento6 páginasCpar ReviewerHana YeppeodaAinda não há avaliações
- ICU General Admission Orders: OthersDocumento2 páginasICU General Admission Orders: OthersHANIMAinda não há avaliações
- Furnace Temperature & PCE ConesDocumento3 páginasFurnace Temperature & PCE ConesAbdullrahman Alzahrani100% (1)
- Agm 1602W-818Documento23 páginasAgm 1602W-818Daniel BauerAinda não há avaliações
- Ward 7Documento14 páginasWard 7Financial NeedsAinda não há avaliações
- Reading Stressful Jobs 1 4Documento4 páginasReading Stressful Jobs 1 4Ivana C. AgudoAinda não há avaliações
- Atom SDDocumento5 páginasAtom SDatomsa shiferaAinda não há avaliações
- Allegro Delivery Shipping Company Employment Application FormDocumento3 páginasAllegro Delivery Shipping Company Employment Application FormshiveshAinda não há avaliações
- Caso Estudio: Reliability Analysis of Power Distribution System. A Case StudyDocumento6 páginasCaso Estudio: Reliability Analysis of Power Distribution System. A Case StudyCarlos HernandezAinda não há avaliações
- Contemp Person Act.1Documento1 páginaContemp Person Act.1Luisa Jane De LunaAinda não há avaliações
- Remedy MidTier Guide 7-5Documento170 páginasRemedy MidTier Guide 7-5martin_wiedmeyerAinda não há avaliações
- Topic 1 - ICT Tools at USP - Theoretical Notes With Google AppsDocumento18 páginasTopic 1 - ICT Tools at USP - Theoretical Notes With Google AppsAvantika PrasadAinda não há avaliações
- PNGRB - Electrical Safety Audit ChecklistDocumento4 páginasPNGRB - Electrical Safety Audit ChecklistKritarth SrivastavAinda não há avaliações
- D. Das and S. Doniach - Existence of A Bose Metal at T 0Documento15 páginasD. Das and S. Doniach - Existence of A Bose Metal at T 0ImaxSWAinda não há avaliações
- Watch One Piece English SubDub Online Free On Zoro - ToDocumento1 páginaWatch One Piece English SubDub Online Free On Zoro - ToSadeusuAinda não há avaliações
- CUET 2022 General Test 6th October Shift 1Documento23 páginasCUET 2022 General Test 6th October Shift 1Dhruv BhardwajAinda não há avaliações
- English 2nd Quarter Week 7 Connotation DenotationDocumento28 páginasEnglish 2nd Quarter Week 7 Connotation DenotationEdward Estrella GuceAinda não há avaliações
- Atlascopco XAHS 175 DD ASL Parts ListDocumento141 páginasAtlascopco XAHS 175 DD ASL Parts ListMoataz SamiAinda não há avaliações