Você também pode gostar
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The 5x5 ProgramDocumento13 páginasThe 5x5 ProgramSMO979Ainda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
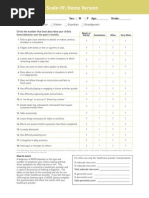
- Screening ADHDDocumento2 páginasScreening ADHDPsiholog Alina Mirela CraiuAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Scope of Human RightsDocumento14 páginasScope of Human RightsJohn Lester Tan100% (2)
- Hypertensive Heart DiseasesDocumento5 páginasHypertensive Heart DiseasesserubimAinda não há avaliações
- Paper Tablets EXPDocumento4 páginasPaper Tablets EXPRosales Gemson Lyster100% (2)
- Usmle Essential BooksDocumento3 páginasUsmle Essential BooksBhavin Choksi33% (3)
- Dri - English - 113 Driver Risk InventoryDocumento6 páginasDri - English - 113 Driver Risk Inventoryminodora100% (1)
- Finally - A Complete Omega 3 Supplement, Only From GNLD!Documento2 páginasFinally - A Complete Omega 3 Supplement, Only From GNLD!Nishit KotakAinda não há avaliações
- SOPs Handling First AidDocumento2 páginasSOPs Handling First AidsridharAinda não há avaliações
- NCM 118 - Lesson 3 (Pulmonary Embolism)Documento4 páginasNCM 118 - Lesson 3 (Pulmonary Embolism)Bobby Christian DuronAinda não há avaliações
- Faktor-Faktor Yang Berhubungan Dengan Kualitas Handover Pasien Di Ruang Rawat Inap Rumah SakitDocumento6 páginasFaktor-Faktor Yang Berhubungan Dengan Kualitas Handover Pasien Di Ruang Rawat Inap Rumah SakitAyu PurbaAinda não há avaliações
- VutaminDocumento66 páginasVutamindyla nabillaAinda não há avaliações
- Work at Height Supervisor Course MandarinDocumento6 páginasWork at Height Supervisor Course Mandarinpanel1bumyj3100% (2)
- Kenya Nutrition Sector-Situation Analysis & Community Consultations PDFDocumento245 páginasKenya Nutrition Sector-Situation Analysis & Community Consultations PDFjtmukui2000Ainda não há avaliações
- 10 Physical and Mental Benefits of BasketballDocumento4 páginas10 Physical and Mental Benefits of BasketballJohn Kenzo NavatoAinda não há avaliações
- Alcohol Treatment CodesDocumento3 páginasAlcohol Treatment CodesMia JacksonAinda não há avaliações
- Philamcare V CADocumento1 páginaPhilamcare V CAOscar E ValeroAinda não há avaliações
- FC Urol (SA) Final Past Papers - 2011 Sept 26-3-2014Documento3 páginasFC Urol (SA) Final Past Papers - 2011 Sept 26-3-2014matentenAinda não há avaliações
- SCD and Hydroxyurea TherapyDocumento29 páginasSCD and Hydroxyurea Therapysamuel waiswaAinda não há avaliações
- COG Chemo Admin GuidelinesDocumento38 páginasCOG Chemo Admin GuidelinesCristina Georgiana ZahariaAinda não há avaliações
- American Indian Reservations: The First Underclass Areas?: Brief History of The Reservation SystemDocumento5 páginasAmerican Indian Reservations: The First Underclass Areas?: Brief History of The Reservation SystemtheactioneerAinda não há avaliações
- Homework PaperDocumento12 páginasHomework Paperapi-509662228Ainda não há avaliações
- Immediate Post-Anaesthesia Recovery 2013Documento20 páginasImmediate Post-Anaesthesia Recovery 2013gythrieAinda não há avaliações
- Reflection 1Documento5 páginasReflection 1api-400554289Ainda não há avaliações
- Nursing Care Plan: Louise O. Reponte BSN-3CDocumento12 páginasNursing Care Plan: Louise O. Reponte BSN-3CLouise MurphyAinda não há avaliações
- Drexel University: Commencement Ceremonies College of MedicineDocumento25 páginasDrexel University: Commencement Ceremonies College of MedicineChimpAinda não há avaliações
- Acetaminophen TylenolDocumento2 páginasAcetaminophen TylenolKristi WrayAinda não há avaliações
- Management of Superficial Phlebitis: Tradition v. ScienceDocumento23 páginasManagement of Superficial Phlebitis: Tradition v. SciencegopscharanAinda não há avaliações
- Notes: Mycobacterium TuberculosisDocumento4 páginasNotes: Mycobacterium TuberculosisAniket SinghAinda não há avaliações
- Astro Forecast Higher Calling WorksheetDocumento22 páginasAstro Forecast Higher Calling WorksheetDaynaAinda não há avaliações