Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Credit Card DetailsDocumento2 páginasCredit Card DetailsAhm Victor83% (6)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Audit - Cash and Cash Equivalents PDFDocumento15 páginasAudit - Cash and Cash Equivalents PDFSiena Farne100% (1)
- Final Project Report On Investment BankingDocumento26 páginasFinal Project Report On Investment BankingSophia Ali78% (9)
- TD Bank Statement USA PDFDocumento7 páginasTD Bank Statement USA PDFrichards emmanuel100% (1)
- Information Sheet - ProbateDocumento9 páginasInformation Sheet - Probateapi-284025444Ainda não há avaliações
- Information Sheet - Ep - IndividualDocumento13 páginasInformation Sheet - Ep - Individualapi-284025444Ainda não há avaliações
- Information Sheet - Ep - CouplesDocumento14 páginasInformation Sheet - Ep - Couplesapi-284025444Ainda não há avaliações
- Information Sheet - LCP - IndividualDocumento14 páginasInformation Sheet - LCP - Individualapi-284025444Ainda não há avaliações
- Guidelines On Risk Appetite Practices For BanksDocumento34 páginasGuidelines On Risk Appetite Practices For BanksPRIME ConsultoresAinda não há avaliações
- Adjusting Entries Until Adjusted Trial Balance - EditedDocumento2 páginasAdjusting Entries Until Adjusted Trial Balance - EditedCINDY LIAN CABILLON100% (2)
- Income Taxes: Sri Lanka Accounting Standard - LKAS 12Documento46 páginasIncome Taxes: Sri Lanka Accounting Standard - LKAS 12Sineth NeththasingheAinda não há avaliações
- WB 2 PDFDocumento4 páginasWB 2 PDFAnnie LamAinda não há avaliações
- FBL Annual Report 2019Documento130 páginasFBL Annual Report 2019Fuaad DodooAinda não há avaliações
- PFP Unit 1 Introduction To Financial PlanningDocumento68 páginasPFP Unit 1 Introduction To Financial PlanningChirag PatilAinda não há avaliações
- Account Statement From 27 Dec 2017 To 27 Jun 2018Documento4 páginasAccount Statement From 27 Dec 2017 To 27 Jun 2018mrcopy xeroxAinda não há avaliações
- The Islamic Gold Dinar Socio-Economic PerspectivesDocumento16 páginasThe Islamic Gold Dinar Socio-Economic PerspectivesmirzalkwAinda não há avaliações
- July 16,2018 Mistake Calling ReportDocumento9 páginasJuly 16,2018 Mistake Calling ReportEesha KanwarAinda não há avaliações
- March 2020 Insight Part IDocumento88 páginasMarch 2020 Insight Part INifezAinda não há avaliações
- Marginal Cost of CapitalDocumento26 páginasMarginal Cost of CapitalSaeedAinda não há avaliações
- Test Bank For Advanced Accounting 14th Edition Joe Ben Hoyle Thomas Schaefer Timothy Doupnik 3Documento71 páginasTest Bank For Advanced Accounting 14th Edition Joe Ben Hoyle Thomas Schaefer Timothy Doupnik 3deborahfritzxmdjcaiknw100% (31)
- Order of Payment: CNC Online Application SystemDocumento1 páginaOrder of Payment: CNC Online Application SystemEva MarquezAinda não há avaliações
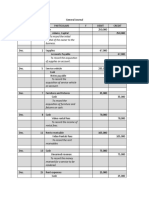
- General JournalDocumento7 páginasGeneral JournalAbigail RososAinda não há avaliações
- Base Dividend PolicyDocumento77 páginasBase Dividend PolicySantosh ChhetriAinda não há avaliações
- 0205 ReposedDocumento45 páginas0205 ReposedLameuneAinda não há avaliações
- CFS ExplanationDocumento13 páginasCFS ExplanationDELFIN, LORENA D.Ainda não há avaliações
- 2015 Trust Technology Buyers Guide PDFDocumento31 páginas2015 Trust Technology Buyers Guide PDFPurnendu MaityAinda não há avaliações
- 0 0 0 1200 0 1200 SGST (0006)Documento1 página0 0 0 1200 0 1200 SGST (0006)Gajanan R GhatageAinda não há avaliações
- Report On Micro FinanceDocumento55 páginasReport On Micro Financearvind.vns14395% (73)
- Cash ManagementDocumento3 páginasCash Managementhae1234Ainda não há avaliações
- PROBLEM NO. 5 - Bank Reconciliation and Amount of Shortage ComputationDocumento2 páginasPROBLEM NO. 5 - Bank Reconciliation and Amount of Shortage Computationelsana philipAinda não há avaliações
- SOUTHWEST AIRWAYS CORPORATION NewDocumento8 páginasSOUTHWEST AIRWAYS CORPORATION NewMelrose UretaAinda não há avaliações
- The Chicago Plan Revisited - 2d Paper IMFDocumento85 páginasThe Chicago Plan Revisited - 2d Paper IMFuser909Ainda não há avaliações
- Nanna MESCOM Payment Receipt-2110405DMCL2787-1949541Documento1 páginaNanna MESCOM Payment Receipt-2110405DMCL2787-1949541Lijesh MathewAinda não há avaliações
- Summer Internship Report (Nitin)Documento28 páginasSummer Internship Report (Nitin)Viswajit100% (1)