Você também pode gostar
- Treating Community Acquired PneumoniaDocumento6 páginasTreating Community Acquired PneumoniaGayuh Candra BuanaAinda não há avaliações
- Dr. D.Y. Patil Vidyapeeth Nursing Lesson Plan Covers Admission to DischargeDocumento3 páginasDr. D.Y. Patil Vidyapeeth Nursing Lesson Plan Covers Admission to DischargeShajinsjAinda não há avaliações
- Surgery PearlsDocumento2 páginasSurgery Pearlspatriciaatan1497Ainda não há avaliações
- Clinical Pathway SC FixDocumento5 páginasClinical Pathway SC Fixnovilusiyana0% (1)
- Wong Worksheet PediaDocumento3 páginasWong Worksheet PediaLecery Sophia WongAinda não há avaliações
- STEER Weaning Protocol 3-2002Documento45 páginasSTEER Weaning Protocol 3-2002patel_vicky87Ainda não há avaliações
- Actual SoapiesDocumento8 páginasActual SoapiesBeverlyn AsparoAinda não há avaliações
- NCP and Focus Charting For PainDocumento3 páginasNCP and Focus Charting For PainArian May MarcosAinda não há avaliações
- Ashley Wolanzyk Concept MapDocumento5 páginasAshley Wolanzyk Concept Mapapi-455796674Ainda não há avaliações
- CP - IPD - Hepatitis Virus AkutDocumento3 páginasCP - IPD - Hepatitis Virus AkutRIyanAinda não há avaliações
- Daily Checklist: 120/80 MMHG 36.5 67 22 1500 CC 1400 CCDocumento53 páginasDaily Checklist: 120/80 MMHG 36.5 67 22 1500 CC 1400 CCJake Yvan DizonAinda não há avaliações
- CP PebDocumento3 páginasCP PebnovaAinda não há avaliações
- Learner'S Worksheet: Clinical RotationDocumento3 páginasLearner'S Worksheet: Clinical RotationLecery Sophia WongAinda não há avaliações
- My Hospital FacilitiesDocumento10 páginasMy Hospital Facilities3E, KENNADY KARUNAKARAN, PRINCEAinda não há avaliações
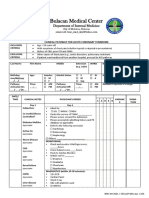
- Clinical Pathway for Acute Coronary Syndrome at Bulacan Medical CenterDocumento7 páginasClinical Pathway for Acute Coronary Syndrome at Bulacan Medical CenterherrerachaimAinda não há avaliações
- PGY 1 Survival Guide MICU 1Documento3 páginasPGY 1 Survival Guide MICU 1Abdulelah MurshidAinda não há avaliações
- PearlsDocumento2 páginasPearlspatriciaatan1497Ainda não há avaliações
- Module 4 OtpDocumento42 páginasModule 4 Otpzack NourAinda não há avaliações
- ACLS Code Blue Checklist FormDocumento8 páginasACLS Code Blue Checklist FormAnastasya Gishella RorongAinda não há avaliações
- Jose Martinez Care PlanDocumento7 páginasJose Martinez Care PlanJulia BrownAinda não há avaliações
- Mechanical Ventilation Weaning Protocol GuideDocumento48 páginasMechanical Ventilation Weaning Protocol GuideJR VendeventerAinda não há avaliações
- Data Collection Form-PainAIRCycleDocumento1 páginaData Collection Form-PainAIRCycleErwin Dela GanaAinda não há avaliações
- Guidelines To Establish Procedural Sedation For GI and OthersDocumento18 páginasGuidelines To Establish Procedural Sedation For GI and OthersayubahriAinda não há avaliações
- Clinical Pathway DSSDocumento7 páginasClinical Pathway DSSfaroexAinda não há avaliações
- Megacode Testing ScenariosDocumento12 páginasMegacode Testing Scenariosmonsalg2502Ainda não há avaliações
- Concept Map PedsDocumento6 páginasConcept Map Pedsapi-498759347Ainda não há avaliações
- ACLS Megacode Testing ScenariosDocumento12 páginasACLS Megacode Testing Scenariosealm10100% (2)
- Heart Failure Clinical Pathway TemplateDocumento3 páginasHeart Failure Clinical Pathway Templategusmarinda fauziahAinda não há avaliações
- Health Failure Clinical PathwayDocumento2 páginasHealth Failure Clinical Pathwayferishandy bagaskaraAinda não há avaliações
- Clinical Pathway - Stroke Without Thrombolytic TherapyDocumento4 páginasClinical Pathway - Stroke Without Thrombolytic TherapysiusiuwidyantoAinda não há avaliações
- Nursing Care Plan Acute PainDocumento3 páginasNursing Care Plan Acute Paindbryant010199% (69)
- Nursing Intervention for Cough and Chest PainDocumento2 páginasNursing Intervention for Cough and Chest PainDiana Anne MarisAinda não há avaliações
- 2022 - Murabito - ES - Resumo - Performance of HPI Inc Bio MarkersDocumento2 páginas2022 - Murabito - ES - Resumo - Performance of HPI Inc Bio MarkersDaniel EllerAinda não há avaliações
- 12ni. Non-Invasive Ventilation (BiPAP) For COPD (University Hospital of South Manchester, Dec 2011)Documento7 páginas12ni. Non-Invasive Ventilation (BiPAP) For COPD (University Hospital of South Manchester, Dec 2011)ManuAinda não há avaliações
- POSToperative 3Documento6 páginasPOSToperative 3joanneAinda não há avaliações
- CP - P - COVID-19 SedangDocumento3 páginasCP - P - COVID-19 SedangRIyanAinda não há avaliações
- 2020 Acls Megacode Testing Scenarios - 2Documento13 páginas2020 Acls Megacode Testing Scenarios - 2Dr. Saqib RazaAinda não há avaliações
- Code Blue Protocols and Multi-Disciplinary Resuscitation TeamsDocumento35 páginasCode Blue Protocols and Multi-Disciplinary Resuscitation TeamsMarsel DonaAinda não há avaliações
- F - KOMED - 13 Soft Tissue TumorDocumento6 páginasF - KOMED - 13 Soft Tissue TumorIvan YosephAinda não há avaliações
- CP - Ipd - DBDDocumento3 páginasCP - Ipd - DBDRIyanAinda não há avaliações
- AHA GWTG-R Code Blue Documentation FormDocumento3 páginasAHA GWTG-R Code Blue Documentation Formrubertusedy100% (3)
- Clinical Pathway Pneumonia RSUD AmpanaDocumento4 páginasClinical Pathway Pneumonia RSUD AmpanaBINA PROGRAMAinda não há avaliações
- Nursing Care Plan for Dengue Hemorrhagic FeverDocumento2 páginasNursing Care Plan for Dengue Hemorrhagic FeverLib Kyron MendozaAinda não há avaliações
- Sample Care Plan Using Case StudyDocumento2 páginasSample Care Plan Using Case StudydestiangrainiAinda não há avaliações
- Clinical Pathway for Asthma in ChildrenDocumento3 páginasClinical Pathway for Asthma in ChildrenHanivan ErwandaAinda não há avaliações
- Daily Assessment Chart ICUDocumento16 páginasDaily Assessment Chart ICUaiman abushahmaAinda não há avaliações
- Bls (BHD) : Dr. Rusdian Nurmadi, Mked (An), SpanDocumento74 páginasBls (BHD) : Dr. Rusdian Nurmadi, Mked (An), SpanDedi Iskandar4549Ainda não há avaliações
- Critical Pathways of Care GuidelineDocumento19 páginasCritical Pathways of Care GuidelineNivedita NivuAinda não há avaliações
- 2021-06-24_Progress Report 2021 Q2 _v1Documento58 páginas2021-06-24_Progress Report 2021 Q2 _v1Da FriendAinda não há avaliações
- SPIROMETRIDocumento27 páginasSPIROMETRIGema Akbar WakhidanaAinda não há avaliações
- HydroceleDocumento10 páginasHydroceleRyan ReAinda não há avaliações
- 2008 Pittcon - Oral Presentation - NanoSpray For CMCDocumento23 páginas2008 Pittcon - Oral Presentation - NanoSpray For CMCmr_jpwalsh8941Ainda não há avaliações
- INTIA, Crisset O. Iii - BN: Submitted byDocumento3 páginasINTIA, Crisset O. Iii - BN: Submitted byCrisset IntiaAinda não há avaliações
- B850 Patient Monitor EvaluationDocumento3 páginasB850 Patient Monitor Evaluationriddhi SutharAinda não há avaliações
- Heart of the Field "Refresher & Nha Certification Quick Notes"No EverandHeart of the Field "Refresher & Nha Certification Quick Notes"Ainda não há avaliações
- Medical Integration Model as it Pertains to Musculoskeletal ConditionsNo EverandMedical Integration Model as it Pertains to Musculoskeletal ConditionsAinda não há avaliações
- Perioperative Pain ManagementNo EverandPerioperative Pain ManagementFelicia CoxAinda não há avaliações
- Step 3 Board-Ready USMLE Junkies: The Must-Have USMLE Step 3 Review CompanionNo EverandStep 3 Board-Ready USMLE Junkies: The Must-Have USMLE Step 3 Review CompanionAinda não há avaliações
- Step 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionNo EverandStep 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionAinda não há avaliações
- Heart Failure Clinical Pathway GuideDocumento7 páginasHeart Failure Clinical Pathway GuidedjizhieeAinda não há avaliações
- Clinical Pathway StrokeDocumento8 páginasClinical Pathway StrokedjizhieeAinda não há avaliações
- Acute Ischemic Stroke PathwayDocumento50 páginasAcute Ischemic Stroke PathwaydjizhieeAinda não há avaliações
- Heart Failure Clinical Pathway GuideDocumento7 páginasHeart Failure Clinical Pathway GuidedjizhieeAinda não há avaliações
- The Effects of Transcranial Direct Current ... (Previ A Impressió) PDFDocumento12 páginasThe Effects of Transcranial Direct Current ... (Previ A Impressió) PDFdjizhieeAinda não há avaliações
- TocDocumento727 páginasTocdjizhiee100% (1)
- International Travel Health ITH - 2009Documento252 páginasInternational Travel Health ITH - 2009djizhieeAinda não há avaliações
- Acute Ischemic Stroke PathwayDocumento50 páginasAcute Ischemic Stroke PathwaydjizhieeAinda não há avaliações
- Clinical Pathway StrokeDocumento8 páginasClinical Pathway StrokedjizhieeAinda não há avaliações
- Public Relation Alert!Documento31 páginasPublic Relation Alert!djizhieeAinda não há avaliações
- 18x24 PosterDocumento1 página18x24 PosterdjizhieeAinda não há avaliações
- Nutrition in The Medical Community (Part 1) - Dr. Khotibuddin - 18 April 2012Documento29 páginasNutrition in The Medical Community (Part 1) - Dr. Khotibuddin - 18 April 2012djizhieeAinda não há avaliações
- All About Partial Seizures PDFDocumento6 páginasAll About Partial Seizures PDFdjizhieeAinda não há avaliações
- CondylomaDocumento4 páginasCondylomaOchabianconeriAinda não há avaliações
- 36x60 Advocate Health Care Vertical TemplateDocumento1 página36x60 Advocate Health Care Vertical TemplatedjizhieeAinda não há avaliações
- Dka Management of Dka in Adults March 20101Documento24 páginasDka Management of Dka in Adults March 20101djizhieeAinda não há avaliações
- ARIA Report 2008Documento196 páginasARIA Report 2008jasbroAinda não há avaliações
- Pathway KeratitisDocumento16 páginasPathway Keratitisdjizhiee100% (1)
- BIMC Adult DKA Protocol 2012Documento5 páginasBIMC Adult DKA Protocol 2012djizhieeAinda não há avaliações
- Dka Guidelines - 2012Documento4 páginasDka Guidelines - 2012djizhieeAinda não há avaliações
- Aria Rhinitis Allergic Pocket GuideDocumento8 páginasAria Rhinitis Allergic Pocket GuideAlfani FajarAinda não há avaliações
- Aria Rhinitis Allergic Pocket GuideDocumento8 páginasAria Rhinitis Allergic Pocket GuideAlfani FajarAinda não há avaliações
- CASP Diagnostic Test Checklist 31.05.13Documento6 páginasCASP Diagnostic Test Checklist 31.05.13itho23Ainda não há avaliações
- DokDocumento1 páginaDokdjizhieeAinda não há avaliações
- MMR SKills Lab 1Documento3 páginasMMR SKills Lab 1djizhieeAinda não há avaliações
- Joint British Diabetes Societies Inpatient Care Group - The Management of Diabetic Ketoacidosis in Adults - Pathway PosterDocumento1 páginaJoint British Diabetes Societies Inpatient Care Group - The Management of Diabetic Ketoacidosis in Adults - Pathway PosterAllison Nadine MarchandAinda não há avaliações
- Joint British Diabetes Societies Inpatient Care Group - The Management of Diabetic Ketoacidosis in Adults - Pathway PosterDocumento1 páginaJoint British Diabetes Societies Inpatient Care Group - The Management of Diabetic Ketoacidosis in Adults - Pathway PosterAllison Nadine MarchandAinda não há avaliações
- Hyperosmolar Hyperglycaemic Non-Ketotic StateDocumento5 páginasHyperosmolar Hyperglycaemic Non-Ketotic StatedjizhieeAinda não há avaliações
- Pre-Op NPO and Traditional Post-Op Diet Advancement: Time To Move OnDocumento7 páginasPre-Op NPO and Traditional Post-Op Diet Advancement: Time To Move OnDaru KristiyonoAinda não há avaliações
- Modified Braden Q ScaleDocumento8 páginasModified Braden Q Scaleapi-122501165Ainda não há avaliações
- Apollo Institute Graduates Ready for Healthcare CareersDocumento60 páginasApollo Institute Graduates Ready for Healthcare CareersboggalaAinda não há avaliações
- TFN - BennerDocumento1 páginaTFN - BennerNikkaDablioAinda não há avaliações
- Cover Letter - Meghan L. ShalvoyDocumento1 páginaCover Letter - Meghan L. ShalvoyMeghan Equality ShalvoyAinda não há avaliações
- CAM ICU Training PDFDocumento32 páginasCAM ICU Training PDFSabrinaMaharaniAinda não há avaliações
- Leff CuckoosDocumento5 páginasLeff CuckoosDominic Roman TringaliAinda não há avaliações
- Faye Glenn AbdellahDocumento3 páginasFaye Glenn AbdellahZia BrionesAinda não há avaliações
- HIMT-Chart 01Documento1 páginaHIMT-Chart 01Shelly NataniaAinda não há avaliações
- Clinical Risk Index For Babies (Crib) Ii Score As A Predictor of Neonatal Mortality Among Low Birth Weight Babies at Kenyatta National HospitalDocumento6 páginasClinical Risk Index For Babies (Crib) Ii Score As A Predictor of Neonatal Mortality Among Low Birth Weight Babies at Kenyatta National HospitalVladBadeaAinda não há avaliações
- S. No. Division Name Purpose Name Fee Paid As Per GSR 1193Documento9 páginasS. No. Division Name Purpose Name Fee Paid As Per GSR 1193VIJAY YADAVAinda não há avaliações
- Maimonides Q2 2019Documento7 páginasMaimonides Q2 2019Jonathan LaMantiaAinda não há avaliações
- Early Christian Era 1Documento2 páginasEarly Christian Era 1mildred alidon100% (1)
- GDM Patient TeachingDocumento2 páginasGDM Patient TeachingBel CortezAinda não há avaliações
- Global Telemedicine and EHealthDocumento6 páginasGlobal Telemedicine and EHealthn1i1Ainda não há avaliações
- ResumeDocumento2 páginasResumeapi-282740776Ainda não há avaliações
- Health Care AgenciesDocumento15 páginasHealth Care AgencieshemihemaAinda não há avaliações
- Assembly Bill No. 2625: Legislative Counsel's DigestDocumento45 páginasAssembly Bill No. 2625: Legislative Counsel's DigestJon OrtizAinda não há avaliações
- Assignment 4Documento3 páginasAssignment 4Jane BiringanAinda não há avaliações
- 1.0. Background of The Study: A Proposed San Jose Del Monte, Bulacan General Hospital Mojares, Lyka M. 16-00853Documento19 páginas1.0. Background of The Study: A Proposed San Jose Del Monte, Bulacan General Hospital Mojares, Lyka M. 16-00853Lyka Mendoza MojaresAinda não há avaliações
- Occupations Jazz ChantDocumento29 páginasOccupations Jazz Chantmieraclampu100% (1)
- Manage Hospital Services CourseDocumento4 páginasManage Hospital Services CourseJobin GeorgeAinda não há avaliações
- Blair Smith Documentation 2012Documento11 páginasBlair Smith Documentation 2012Eni SartikaAinda não há avaliações
- Scope of Nle908Documento244 páginasScope of Nle908ericAinda não há avaliações
- Christine Piper - After Darkness (Extract)Documento34 páginasChristine Piper - After Darkness (Extract)Allen & Unwin100% (3)
- VAKRATUNDA HOSPITAL PATIENT POLICYDocumento11 páginasVAKRATUNDA HOSPITAL PATIENT POLICYVIKRAM PATOLE100% (1)
- Daftar Pustaka-MendeleyDocumento3 páginasDaftar Pustaka-Mendeleynurafiat175Ainda não há avaliações
- Manual Therapies Osteopathy & ChiropracticDocumento28 páginasManual Therapies Osteopathy & Chiropractickotza100% (1)
- 2011 Article 162 PDFDocumento8 páginas2011 Article 162 PDFJ.J.Ainda não há avaliações
- Kollabio - Health360 Pitch DeckDocumento18 páginasKollabio - Health360 Pitch Deckshiplet100% (1)
- Relative pronoun and participle clause quizDocumento4 páginasRelative pronoun and participle clause quizΓΙΑΝΝΗΣ ΚΟΝΔΥΛΗΣ100% (1)