Você também pode gostar
- Food Manager Certification Study GuideDocumento15 páginasFood Manager Certification Study GuideSharon KuAinda não há avaliações
- Low Oxalate Diet Guide to Prevent Kidney StonesDocumento5 páginasLow Oxalate Diet Guide to Prevent Kidney StonesCarlos Santos100% (2)
- A Journey To The Single MaltsDocumento14 páginasA Journey To The Single MaltsSiddhartha TripathiAinda não há avaliações
- Carcinoma of Penis: DR Hitesh Patel Associate Professor Surgery Department GMERS Medical College, GotriDocumento55 páginasCarcinoma of Penis: DR Hitesh Patel Associate Professor Surgery Department GMERS Medical College, Gotrihitesh3150% (1)
- Healthy VegetarianDocumento28 páginasHealthy VegetarianMihai GodeanuAinda não há avaliações
- Managing Chronic PainDocumento2 páginasManaging Chronic PainMilenaSpasovskaAinda não há avaliações
- Chronic ConstipationDocumento25 páginasChronic ConstipationhandikaAinda não há avaliações
- Fasting-and-CancerDocumento3 páginasFasting-and-CancerfrancoAinda não há avaliações
- Probiotics and Constipation Mechanisms of Action Evidence For Effectiveness and Utilisation by Patients and Healthcare ProfessionalsDocumento11 páginasProbiotics and Constipation Mechanisms of Action Evidence For Effectiveness and Utilisation by Patients and Healthcare ProfessionalsnganhaAinda não há avaliações
- Konstipasi Aha AsaDocumento7 páginasKonstipasi Aha AsaClaudia TiffanyAinda não há avaliações
- An Approach To The Diagnosis and Management of Rome IV Functional Disorders of Chronic ConstipationDocumento9 páginasAn Approach To The Diagnosis and Management of Rome IV Functional Disorders of Chronic ConstipationLianita HoAinda não há avaliações
- Diagnosis and Treatment of Chronic Constipation - A European PerspectiveDocumento14 páginasDiagnosis and Treatment of Chronic Constipation - A European Perspectiveadinny julmizaAinda não há avaliações
- Tramonte1997 Article TheTreatmentOfChronicConstipatDocumento10 páginasTramonte1997 Article TheTreatmentOfChronicConstipatAndreea PopescuAinda não há avaliações
- Chronic Diarrhea PDFDocumento5 páginasChronic Diarrhea PDFnaryAinda não há avaliações
- Managing Chronic Diarrhea With Colorectal Cancer: Symptom Management SeriesDocumento7 páginasManaging Chronic Diarrhea With Colorectal Cancer: Symptom Management SeriescindyAinda não há avaliações
- Triagem EspenDocumento7 páginasTriagem EspenGogo RouAinda não há avaliações
- Constipacion - 2017 - Regimen Intestinal - EnseñanzaDocumento2 páginasConstipacion - 2017 - Regimen Intestinal - EnseñanzaManuel MontellanosAinda não há avaliações
- Tuck_et_al-2018-Neurogastroenterology_&_MotilityDocumento20 páginasTuck_et_al-2018-Neurogastroenterology_&_MotilityESTHEFANE SILVAAinda não há avaliações
- Irritable Bowel SyndromeDocumento13 páginasIrritable Bowel SyndromeYara Olalde CancinoAinda não há avaliações
- (Mayo Clinic Proceedings, Jan 2022) - 75 Year Old Woman With Abdominal Pain and ConstipationDocumento5 páginas(Mayo Clinic Proceedings, Jan 2022) - 75 Year Old Woman With Abdominal Pain and ConstipationNigelyulAinda não há avaliações
- 2017-Diareea Cronica PDFDocumento15 páginas2017-Diareea Cronica PDFAnastasia NicuAinda não há avaliações
- Chronic Diarrhea Diagnosis and ManagementDocumento15 páginasChronic Diarrhea Diagnosis and ManagementNicolas BustamanteAinda não há avaliações
- Best Management of Irritable Bowel SyndromeDocumento13 páginasBest Management of Irritable Bowel SyndromeIsaac Martinez ArevaloAinda não há avaliações
- Harrisons Principles of Internal Medicine 21st Edition Vol 1 Vol Split PDF 1694700703964Documento73 páginasHarrisons Principles of Internal Medicine 21st Edition Vol 1 Vol Split PDF 1694700703964Clorinda RodriguezAinda não há avaliações
- Cocca 28 190Documento8 páginasCocca 28 190SYIFA MAULA NUR PADILAHAinda não há avaliações
- Review: Treatment of Constipation in Older PeopleDocumento8 páginasReview: Treatment of Constipation in Older PeopleMohd ZulAmirulAinda não há avaliações
- Pharmacotherapy Considerations in Palliative Care: Learning ObjectivesDocumento19 páginasPharmacotherapy Considerations in Palliative Care: Learning ObjectivesMajed Mubarak Shannan AlzahraniAinda não há avaliações
- Treating Obesity Seriously. When Recommendations For As Recomendações Por Um Estilo de Vida São Confrontados Pelas Adaptações BiológicasDocumento3 páginasTreating Obesity Seriously. When Recommendations For As Recomendações Por Um Estilo de Vida São Confrontados Pelas Adaptações BiológicasClaudia GuimarãesAinda não há avaliações
- Constipation For CancerDocumento15 páginasConstipation For Cancerpalomazul007Ainda não há avaliações
- 2018 PHYS REV Ingestão Alimentar e Comportamento Alimentar Depois de Cirurgia BariátricaDocumento29 páginas2018 PHYS REV Ingestão Alimentar e Comportamento Alimentar Depois de Cirurgia BariátricaLeonardoCampanelliAinda não há avaliações
- Review: Nutrition On Chronic Liver Diseases: Kadayifci Fatma Zehra and Kadayifci AbdurrahmanDocumento4 páginasReview: Nutrition On Chronic Liver Diseases: Kadayifci Fatma Zehra and Kadayifci AbdurrahmanFlora PopaAinda não há avaliações
- Irritable Bowel Syndrome With Diarrhea Treatment Is A Work in ProgressDocumento11 páginasIrritable Bowel Syndrome With Diarrhea Treatment Is A Work in ProgressCamila CharryAinda não há avaliações
- BMJ 2020 063613.fullDocumento8 páginasBMJ 2020 063613.fullSahira DarAinda não há avaliações
- Clinchem 0118Documento12 páginasClinchem 0118laura correaAinda não há avaliações
- 1252-Article Text-5341-2-10-20200212Documento6 páginas1252-Article Text-5341-2-10-20200212Lizette AntonioAinda não há avaliações
- Wolfe Et Al., 2016 - BSDocumento23 páginasWolfe Et Al., 2016 - BSJulia SCAinda não há avaliações
- Malnourished?: Is This PatientDocumento5 páginasMalnourished?: Is This PatientJason WongAinda não há avaliações
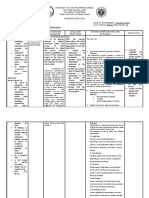
- University of The Philippines ManilaDocumento6 páginasUniversity of The Philippines ManilaTessa Lisbury SteakAinda não há avaliações
- Safety and Feasibility of Intermittent Fasting During Chemotherapy For Breast Cancer: A Review of The LiteratureDocumento11 páginasSafety and Feasibility of Intermittent Fasting During Chemotherapy For Breast Cancer: A Review of The LiteratureMargaret ReedAinda não há avaliações
- Abdominal Bloating: Is It All in The Gas?Documento6 páginasAbdominal Bloating: Is It All in The Gas?danny17phAinda não há avaliações
- Case Series in Lifestyle Medicine: A Team Approach To Behavior ChangesDocumento10 páginasCase Series in Lifestyle Medicine: A Team Approach To Behavior ChangesSgantzos MarkosAinda não há avaliações
- The Effects of Gastric Bypass Surgery On Drug Absorption and PharmacokineticsDocumento15 páginasThe Effects of Gastric Bypass Surgery On Drug Absorption and PharmacokineticsAndrés MaldonadoAinda não há avaliações
- Choosing The Most Appropriate Biologic Therapy For Crohn's Disease According To Concomitant Extra-Intestinal Manifestations, Comorbidities, or Physiologic ConditionsDocumento44 páginasChoosing The Most Appropriate Biologic Therapy For Crohn's Disease According To Concomitant Extra-Intestinal Manifestations, Comorbidities, or Physiologic ConditionsBernadett FarkasAinda não há avaliações
- DCR 2016 Constipation, Evaluation and Management ofDocumento14 páginasDCR 2016 Constipation, Evaluation and Management ofrisewfAinda não há avaliações
- 2021 Behavioral and Diet Therapies in Integrated Care For Patients With IBSDocumento16 páginas2021 Behavioral and Diet Therapies in Integrated Care For Patients With IBSanonAinda não há avaliações
- Improving End of Life CareDocumento9 páginasImproving End of Life CareM_LXAinda não há avaliações
- Fast Hug FaithDocumento4 páginasFast Hug FaithHenrique Yuji Watanabe SilvaAinda não há avaliações
- Diarrhea For CancerDocumento17 páginasDiarrhea For Cancerpalomazul007Ainda não há avaliações
- Mdy 148Documento15 páginasMdy 148andiAinda não há avaliações
- The Role of Lifestyle Changes in The Management of Chronic Liver DiseaseDocumento7 páginasThe Role of Lifestyle Changes in The Management of Chronic Liver DiseaseLila FathiaAinda não há avaliações
- Management of GIDocumento24 páginasManagement of GIrluisleoAinda não há avaliações
- Managing Opioid-Induced ConstipationDocumento9 páginasManaging Opioid-Induced ConstipationTom Rue100% (1)
- Practice: Infectious Diarrhea: When To Test and When To TreatDocumento7 páginasPractice: Infectious Diarrhea: When To Test and When To TreatteryjAinda não há avaliações
- J of Gastro and Hepatol - 2013 - SchillerDocumento20 páginasJ of Gastro and Hepatol - 2013 - Schillerzakiah11Ainda não há avaliações
- Nejmcp 2114026Documento10 páginasNejmcp 2114026Cristina Adriana PopaAinda não há avaliações
- Tratamiento de La GastroparesiaDocumento7 páginasTratamiento de La GastroparesiaAnnabelle YagualAinda não há avaliações
- Patterns of Dying: Palliative Care For Non-Malignant DiseaseDocumento6 páginasPatterns of Dying: Palliative Care For Non-Malignant Diseasefabian dionAinda não há avaliações
- Gutjnl 2011 300563.fullDocumento15 páginasGutjnl 2011 300563.fullVince Daniel VillalbaAinda não há avaliações
- Article Bayhon WardDocumento7 páginasArticle Bayhon WardJULIANNE BAYHONAinda não há avaliações
- Diagnostic Approach To Chronic Constipation in Adults: Namirah Jamshed, MD Zone-En Lee, MD and Kevin W. Olden, MDDocumento8 páginasDiagnostic Approach To Chronic Constipation in Adults: Namirah Jamshed, MD Zone-En Lee, MD and Kevin W. Olden, MDwilson koresAinda não há avaliações
- Hyperglycemic CrisisDocumento9 páginasHyperglycemic CrisisRoberto López MataAinda não há avaliações
- Hepatitis B Vaccination, Screening, and Linkage To Care - Best Practice Advice From The American College of Physicians and The Centers For Disease Control and PreventionDocumento12 páginasHepatitis B Vaccination, Screening, and Linkage To Care - Best Practice Advice From The American College of Physicians and The Centers For Disease Control and PreventionRoberto López MataAinda não há avaliações
- Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Synopsis of The 2017 American College of Cardiology:American Heart Association Hypertension GuidelineDocumento10 páginasPrevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Synopsis of The 2017 American College of Cardiology:American Heart Association Hypertension GuidelineRoberto López MataAinda não há avaliações
- 2017 ACC Expert Consensus Decision Pathway For Optimization of Heart Failure TreatmentDocumento30 páginas2017 ACC Expert Consensus Decision Pathway For Optimization of Heart Failure TreatmentRoberto López MataAinda não há avaliações
- Atrial Fibrillation and HypertensionDocumento17 páginasAtrial Fibrillation and HypertensionRoberto López MataAinda não há avaliações
- Diagnosis and Treatment of HyperkalemiaDocumento9 páginasDiagnosis and Treatment of HyperkalemiaRoberto López MataAinda não há avaliações
- HTN Emergencies and UrgenciesDocumento14 páginasHTN Emergencies and UrgenciesRoberto López MataAinda não há avaliações
- Top 10 Myths Regarding The Diagnosis and Treatment of CellulitisDocumento8 páginasTop 10 Myths Regarding The Diagnosis and Treatment of CellulitisRoberto López MataAinda não há avaliações
- ADA 2018 Diabetes CareDocumento150 páginasADA 2018 Diabetes CareRoberto López Mata100% (1)
- Update On The Management of Venous ThromboembolismDocumento8 páginasUpdate On The Management of Venous ThromboembolismRoberto López MataAinda não há avaliações
- Necrotizing Soft-Tissue InfectionsDocumento13 páginasNecrotizing Soft-Tissue InfectionsRoberto López MataAinda não há avaliações
- Sudden Cardiac Arrest During Participation in Competitive SportsDocumento11 páginasSudden Cardiac Arrest During Participation in Competitive SportsRoberto López MataAinda não há avaliações
- Best Clinical Practice: AnaphylaxisDocumento6 páginasBest Clinical Practice: AnaphylaxisputriAinda não há avaliações
- Uric Acid Is A Strong Risk Marker For Developing Hypertension From PrehypertensionDocumento16 páginasUric Acid Is A Strong Risk Marker For Developing Hypertension From PrehypertensionRoberto López MataAinda não há avaliações
- Fluid Therapy Options and Rational SelectionDocumento13 páginasFluid Therapy Options and Rational SelectionRoberto López MataAinda não há avaliações
- Pathophysiology of Septic ShockDocumento19 páginasPathophysiology of Septic ShockRoberto López MataAinda não há avaliações
- The Role of Nitroglycerin and Other Nitrogen Oxides in Cardiovascular TherapeuticsDocumento18 páginasThe Role of Nitroglycerin and Other Nitrogen Oxides in Cardiovascular TherapeuticsRoberto López MataAinda não há avaliações
- The Use of Cephalosporins in Penicillin-Allergic Patients - A Literature ReviewDocumento9 páginasThe Use of Cephalosporins in Penicillin-Allergic Patients - A Literature ReviewRoberto López MataAinda não há avaliações
- 2015 ESC Guidelines For The Diagnosis and Management of Pericardial DiseasesDocumento44 páginas2015 ESC Guidelines For The Diagnosis and Management of Pericardial DiseasesRoberto López MataAinda não há avaliações
- Rivaroxaban Vs Warfarin Sodium in The Ultra-Early Period After Atrial Fibrillation-Related Mild Ischemic StrokeDocumento10 páginasRivaroxaban Vs Warfarin Sodium in The Ultra-Early Period After Atrial Fibrillation-Related Mild Ischemic StrokeRoberto López MataAinda não há avaliações
- The Dark Sides of Fuid Administration in The Critically Ill PatientDocumento3 páginasThe Dark Sides of Fuid Administration in The Critically Ill PatientRoberto López MataAinda não há avaliações
- Diuretic Treatment in Heart FailureDocumento12 páginasDiuretic Treatment in Heart FailureRoberto López Mata100% (1)
- A Test in Context - D-DimerDocumento10 páginasA Test in Context - D-DimerRoberto López MataAinda não há avaliações
- Effects on the Incidence of Cardiovascular Events of the Addition of Pioglitazone Versus Sulfonylureas in Patients With Type 2 Diabetes Inadequately Controlled With Metformin (TOSCA.it)- A Randomised, Multicentre TrialDocumento11 páginasEffects on the Incidence of Cardiovascular Events of the Addition of Pioglitazone Versus Sulfonylureas in Patients With Type 2 Diabetes Inadequately Controlled With Metformin (TOSCA.it)- A Randomised, Multicentre TrialRoberto López MataAinda não há avaliações
- Effects of Acarbose On Cardiovascular and Diabetes Outcomes in Patients With Coronary Heart Disease and Impaired Glucose Tolerance (ACE) - A Randomised, Double-Blind, Placebo-Controlled TrialDocumento10 páginasEffects of Acarbose On Cardiovascular and Diabetes Outcomes in Patients With Coronary Heart Disease and Impaired Glucose Tolerance (ACE) - A Randomised, Double-Blind, Placebo-Controlled TrialRoberto López MataAinda não há avaliações
- Synopsis of The 2017 U.S. Department of Veterans Affairs: Management of Type 2 Diabetes MellitusDocumento10 páginasSynopsis of The 2017 U.S. Department of Veterans Affairs: Management of Type 2 Diabetes MellitusRoberto López MataAinda não há avaliações
- Evaluation and Management of Lower-Extremity UlcersDocumento9 páginasEvaluation and Management of Lower-Extremity UlcersRoberto López MataAinda não há avaliações
- Acute Monocular Vision LossDocumento9 páginasAcute Monocular Vision LossRoberto López MataAinda não há avaliações
- Dual Antithrombotic Therapy With Dabigatran After PCI in Atrial FibrillationDocumento12 páginasDual Antithrombotic Therapy With Dabigatran After PCI in Atrial FibrillationRoberto López MataAinda não há avaliações
- Chapter 01: Drug Definitions, Standards, and Information Sources Willihnganz: Clayton's Basic Pharmacology For Nurses, 18th EditionDocumento4 páginasChapter 01: Drug Definitions, Standards, and Information Sources Willihnganz: Clayton's Basic Pharmacology For Nurses, 18th Editioncharlie johnsonAinda não há avaliações
- International Journal of Innovative Pharmaceutical Research: Ophthalmic Delivery System For Dexamethasone: An OverviewDocumento5 páginasInternational Journal of Innovative Pharmaceutical Research: Ophthalmic Delivery System For Dexamethasone: An OverviewGufron MustofaAinda não há avaliações
- Merck's Formulation HandbookDocumento112 páginasMerck's Formulation HandbookAhmad Talaat100% (2)
- Annexure-I Company Requisitions ListDocumento5 páginasAnnexure-I Company Requisitions ListShweAinda não há avaliações
- Insecticidal Activity of Castanospermum Australe Against Stored Grain Pest Callosobruchus AnalisDocumento3 páginasInsecticidal Activity of Castanospermum Australe Against Stored Grain Pest Callosobruchus AnalisIOSR Journal of PharmacyAinda não há avaliações
- Antibiotic Classification & Mechanism - Basic Science - OrthobulletsDocumento9 páginasAntibiotic Classification & Mechanism - Basic Science - OrthobulletsHossam Elden Helmy HaridyAinda não há avaliações
- Career PortfolioDocumento12 páginasCareer PortfolioNatasya Fariha ShafiiAinda não há avaliações
- A Report On Beximco Pharmaceuticals LTDDocumento14 páginasA Report On Beximco Pharmaceuticals LTDAli Asgor RatonAinda não há avaliações
- Pharmacovigilance Related Questions - 1585456120320Documento10 páginasPharmacovigilance Related Questions - 1585456120320Saravanan RamAinda não há avaliações
- FLABEX CAPSULES AYURVEDIC WEIGHT LOSS MEDICINEDocumento3 páginasFLABEX CAPSULES AYURVEDIC WEIGHT LOSS MEDICINEhk_scribdAinda não há avaliações
- Pallava Template For Oral Presentation GeneralDocumento20 páginasPallava Template For Oral Presentation GeneralVijay BhaskarAinda não há avaliações
- Medication Administration TimesDocumento3 páginasMedication Administration TimesBenjel AndayaAinda não há avaliações
- Drug StudyDocumento41 páginasDrug StudyVecky TolentinoAinda não há avaliações
- Jurubeba PowderDocumento2 páginasJurubeba PowderHerman Augusto SchmitzAinda não há avaliações
- The Jere Beasley Report, Feb. 2014Documento40 páginasThe Jere Beasley Report, Feb. 2014Beasley AllenAinda não há avaliações
- Drug Information ResourcesDocumento27 páginasDrug Information ResourcesMA Masum HossainAinda não há avaliações
- Critical Appraisal Jurnal Asam Traneksamat Pada MelasmaDocumento4 páginasCritical Appraisal Jurnal Asam Traneksamat Pada MelasmaMsrirrrAinda não há avaliações
- 17 Chemicals and Fertilizers 21Documento100 páginas17 Chemicals and Fertilizers 21JAYESH6Ainda não há avaliações
- Experiential Pharmacy Practice in Institutional Pharmacy: Module 1: Part 2Documento27 páginasExperiential Pharmacy Practice in Institutional Pharmacy: Module 1: Part 2levi pinedaAinda não há avaliações
- FluidsHndbkPreview PDFDocumento29 páginasFluidsHndbkPreview PDFprematellieAinda não há avaliações
- ATC/DDD Classification (Temporary)Documento8 páginasATC/DDD Classification (Temporary)selvi aklailia rosaAinda não há avaliações
- Phardose Lab Aromatic Water Dakin SDocumento5 páginasPhardose Lab Aromatic Water Dakin SJaica Mangurali TumulakAinda não há avaliações
- Ace Lofe Nac ContainingDocumento16 páginasAce Lofe Nac ContainingUmeerAinda não há avaliações
- PL - Grosir - 12-08-2023Documento29 páginasPL - Grosir - 12-08-2023Fanteri Aji DharmaAinda não há avaliações
- Paracetamol and CodeineDocumento4 páginasParacetamol and CodeineBilal MasoodAinda não há avaliações
- Bronchial AsthmaDocumento40 páginasBronchial Asthmasamson bd mokuntil100% (1)
- GVP Module II Pharmacovigilance System Master File Rev 2 - en PDFDocumento20 páginasGVP Module II Pharmacovigilance System Master File Rev 2 - en PDFBipin Bhagath.LAinda não há avaliações
- Product Profiling and ManufacturingDocumento16 páginasProduct Profiling and ManufacturingPriyanka RawoolAinda não há avaliações
- MCQ 2 - PharmacodynamicsDocumento5 páginasMCQ 2 - PharmacodynamicsHillary Nguyen100% (3)
- Loperamide PDFDocumento2 páginasLoperamide PDFaguerro100% (1)