Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- BURGER KING Market EntryDocumento43 páginasBURGER KING Market EntryVeronika KozlovetsAinda não há avaliações
- La Calle Tacos & CantinaDocumento20 páginasLa Calle Tacos & CantinaIng Dionicio SeguraAinda não há avaliações
- Moonspinners by Mary Stewart (C) 1962, The - The Moonspinners (V. 3)Documento151 páginasMoonspinners by Mary Stewart (C) 1962, The - The Moonspinners (V. 3)Neto HernándezAinda não há avaliações
- Extension Project ReportDocumento19 páginasExtension Project ReportAgriHermitAinda não há avaliações
- HanjeliDocumento8 páginasHanjeliRirin Natasia SitinjakAinda não há avaliações
- Director of Marketing and Public RelationsDocumento3 páginasDirector of Marketing and Public Relationsapi-77855168Ainda não há avaliações
- Zoology ProjectDocumento20 páginasZoology ProjectUMESH WADASKARAinda não há avaliações
- Exposicion de Ingles Los PollosDocumento8 páginasExposicion de Ingles Los Pollosana maria saltosAinda não há avaliações
- Demigods & Magicians - The Son of Sobek - ExcerpDocumento8 páginasDemigods & Magicians - The Son of Sobek - Excerpmsreeat60% (5)
- Patanjali Product List in Excel Aug 2017Documento6 páginasPatanjali Product List in Excel Aug 2017Vijay MeharwadeAinda não há avaliações
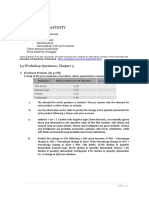
- L3. Elasticity - CH 3, Questions (Teacher)Documento5 páginasL3. Elasticity - CH 3, Questions (Teacher)shikha ramdanyAinda não há avaliações
- The Legendary Moonlight Sculptor Volume 12 PDFDocumento218 páginasThe Legendary Moonlight Sculptor Volume 12 PDFFey YshalAinda não há avaliações
- Admissions Rules and Regulations General RulesDocumento4 páginasAdmissions Rules and Regulations General RulesShehnaz BaigAinda não há avaliações
- Health Assessment QuizDocumento24 páginasHealth Assessment QuizJoyzoey95% (19)
- Poverty of India (By Dadabhai Naoroji)Documento246 páginasPoverty of India (By Dadabhai Naoroji)somebody535Ainda não há avaliações
- Diverse Group of Adventurers and Locals Fill TavernDocumento3 páginasDiverse Group of Adventurers and Locals Fill TavernRichardAinda não há avaliações
- 7 30 14Documento24 páginas7 30 14greercitizenAinda não há avaliações
- STS Module 2Documento8 páginasSTS Module 2Gladys ChengAinda não há avaliações
- Can I Take Your OrderDocumento2 páginasCan I Take Your OrderSarah MahonAinda não há avaliações
- IcelleDocumento9 páginasIcelleMaricel LimAinda não há avaliações
- Ojt ReportDocumento52 páginasOjt ReportJaySimon83% (6)
- 2014 Effie WinnersDocumento16 páginas2014 Effie WinnersalbaxitoAinda não há avaliações
- Day On The FarmDocumento1 páginaDay On The FarmRizi Mae CodalAinda não há avaliações
- Topic 16Documento1 páginaTopic 16Nguyễn HuyềnAinda não há avaliações
- Don Bosco Splendid Home 1 Terminal Examination-2017 Class-II MathsDocumento5 páginasDon Bosco Splendid Home 1 Terminal Examination-2017 Class-II Mathsproodoot100% (1)
- Marele Dictionar Englez-Roman de ExpresiiDocumento22 páginasMarele Dictionar Englez-Roman de ExpresiiOana Dorofte100% (1)
- Got Milk: Branding A CommodityDocumento20 páginasGot Milk: Branding A CommodityTabish Ahmed HashmiAinda não há avaliações
- AWKENOX - Catalog 2015-16 PDFDocumento59 páginasAWKENOX - Catalog 2015-16 PDFEchmumbai adminAinda não há avaliações
- Characteristics of ResearchDocumento23 páginasCharacteristics of ResearchJoana CabatañaAinda não há avaliações
- 3m Petrifilm Salmonella Express System AoacDocumento3 páginas3m Petrifilm Salmonella Express System AoacAngel CasierraAinda não há avaliações