Você também pode gostar
- Stevens Johnson SyndromeDocumento14 páginasStevens Johnson SyndromeGaemkyulyea KVn100% (1)
- Coxsackie Virus: Hand, Foot and Mouth DiseaseDocumento36 páginasCoxsackie Virus: Hand, Foot and Mouth DiseaseSuhazeli AbdullahAinda não há avaliações
- Paroxysmal Nocturnal Hemoglobinuria Case StudyDocumento87 páginasParoxysmal Nocturnal Hemoglobinuria Case Studyrachael100% (4)
- Case - Steven Johnson'sDocumento72 páginasCase - Steven Johnson'sLea Marie SalazarAinda não há avaliações
- HEMA 1 QUIZ multiple choice and matching practiceDocumento2 páginasHEMA 1 QUIZ multiple choice and matching practiceChristian John Mabalot CarilloAinda não há avaliações
- Guideline For TransesDocumento1 páginaGuideline For TransesHannahAinda não há avaliações
- Laboratory Safety and Microscopy Principles for BACT211Documento86 páginasLaboratory Safety and Microscopy Principles for BACT211kurotsukki todorokiAinda não há avaliações
- Causes and Treatment of Acute Poststreptococcal GlomerulonephritisDocumento6 páginasCauses and Treatment of Acute Poststreptococcal GlomerulonephritisMohamed ZiadaAinda não há avaliações
- URINALYSIS TESTING GUIDEDocumento6 páginasURINALYSIS TESTING GUIDEThanz Pamela Gargueña Guisihan100% (1)
- Nursing Student Masters Blood Transfusion SkillsDocumento2 páginasNursing Student Masters Blood Transfusion Skillscaitie miracleAinda não há avaliações
- Clinical Chemistry 1: Key Concepts and Laboratory AnalysesDocumento26 páginasClinical Chemistry 1: Key Concepts and Laboratory AnalysespikachuAinda não há avaliações
- Hirschsprung's Disease Signs, Causes and Nursing CareDocumento7 páginasHirschsprung's Disease Signs, Causes and Nursing CareEdilyn BalicaoAinda não há avaliações
- POTTs Disease PathoDocumento3 páginasPOTTs Disease PathoEdgel QuidolesAinda não há avaliações
- Egg Hunting GuideDocumento6 páginasEgg Hunting GuidesmilingfroggyAinda não há avaliações
- Chapter 38 - Pediatric and Geriatric HematologyDocumento3 páginasChapter 38 - Pediatric and Geriatric HematologyNathaniel Sim100% (2)
- SCHISTOSOMIASISDocumento3 páginasSCHISTOSOMIASISsands32Ainda não há avaliações
- Prothrombin Time: Reference Range, Interpretation, Collection and ..Documento3 páginasProthrombin Time: Reference Range, Interpretation, Collection and ..Francis Polycarp DiazAinda não há avaliações
- Micro Lab Prac - PDCR PDFDocumento10 páginasMicro Lab Prac - PDCR PDFPatti Danielle Referente50% (2)
- Culture Media FinalDocumento25 páginasCulture Media FinalRaghu KumarAinda não há avaliações
- Giardiasis and FecalysisDocumento2 páginasGiardiasis and Fecalysiskmpg11Ainda não há avaliações
- CC1 Lab Fin V2Documento22 páginasCC1 Lab Fin V2Melody PardilloAinda não há avaliações
- Rheumatic Heart DiseaseDocumento30 páginasRheumatic Heart DiseasejustinahorroAinda não há avaliações
- Immunology and Serology Course OutlineDocumento4 páginasImmunology and Serology Course OutlineLynn CorreaAinda não há avaliações
- PMLS1 Lesson 3Documento8 páginasPMLS1 Lesson 3John Daniel AriasAinda não há avaliações
- Hematologic DisordersDocumento40 páginasHematologic DisordersMary Grace LeronAinda não há avaliações
- Clinical Parasitology Mid Term TransDocumento11 páginasClinical Parasitology Mid Term TransBelle LatAinda não há avaliações
- Nursing Theory to Practice SkillsDocumento10 páginasNursing Theory to Practice SkillsCristel CailaoAinda não há avaliações
- 6 Ra 1517Documento56 páginas6 Ra 1517Jay Andrea Vea Dayuday-IsraelAinda não há avaliações
- Laboratory Tests for Hemostasis EvaluationDocumento5 páginasLaboratory Tests for Hemostasis EvaluationCMLAinda não há avaliações
- Sop - ObgynDocumento5 páginasSop - ObgynanalourdesbonitaAinda não há avaliações
- Fecalysis: Tests on Stool Samples to Diagnose Digestive ConditionsDocumento2 páginasFecalysis: Tests on Stool Samples to Diagnose Digestive ConditionsHan SoloAinda não há avaliações
- SLU School of Medicine Report on PEM CasesDocumento10 páginasSLU School of Medicine Report on PEM CasesJeffrey RamosAinda não há avaliações
- FHN MODULE1 (PART 1) OVERVIEW of COMMUNITY HEALTH NURSING-1 PDFDocumento5 páginasFHN MODULE1 (PART 1) OVERVIEW of COMMUNITY HEALTH NURSING-1 PDFKyedae ShymkoAinda não há avaliações
- Parasitology ProtozoaDocumento132 páginasParasitology ProtozoaMikay Cutaran0% (1)
- 1335687089.75523 Lab PracticalHematologyManualDocumento62 páginas1335687089.75523 Lab PracticalHematologyManualAgustín Manriquez EspinozaAinda não há avaliações
- UrinalysisDocumento120 páginasUrinalysisKate Alyssa Caton100% (1)
- Malarial ParasitesDocumento5 páginasMalarial ParasitesZette ArañaAinda não há avaliações
- Biochemical TestDocumento13 páginasBiochemical TestSusi100% (1)
- Parasites and Protozoa: Morphology, Life Cycles, Diseases and TreatmentsDocumento47 páginasParasites and Protozoa: Morphology, Life Cycles, Diseases and TreatmentsKim Delaney MadridAinda não há avaliações
- Our Lady of Fatima University Medical Laboratory Science Principles NotesDocumento22 páginasOur Lady of Fatima University Medical Laboratory Science Principles NotesKat JornadalAinda não há avaliações
- URINALYSISDocumento63 páginasURINALYSISMedah Naserian100% (2)
- Abo Blood Group SystemDocumento10 páginasAbo Blood Group SystemMariel AbatayoAinda não há avaliações
- Acute Myeloid Leukemia in PediatricDocumento43 páginasAcute Myeloid Leukemia in PediatricSari HestiyariniAinda não há avaliações
- Rheumatic Heart Disease and Hydatidiform Mole CaseDocumento90 páginasRheumatic Heart Disease and Hydatidiform Mole CaseGhra CiousAinda não há avaliações
- Blood Transfusion Guidelines PDFDocumento21 páginasBlood Transfusion Guidelines PDFEmhemed Amer Tabib100% (2)
- Parasitology 2019 Lecture Notes: Prepared By: Ariane T. Laranang, RMT, MT (Ascpi), MSMTDocumento39 páginasParasitology 2019 Lecture Notes: Prepared By: Ariane T. Laranang, RMT, MT (Ascpi), MSMTShane Ann RodriguezAinda não há avaliações
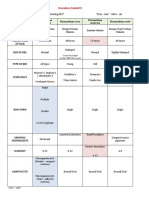
- Pathognomonic Signs of Communicable Diseases: JJ8009 Health & NutritionDocumento2 páginasPathognomonic Signs of Communicable Diseases: JJ8009 Health & NutritionMauliza Resky NisaAinda não há avaliações
- CSF Analysis GuideDocumento248 páginasCSF Analysis GuideGennelyn Ross Delos Reyes0% (1)
- PCAP Report ClerkshipDocumento54 páginasPCAP Report ClerkshipMichelleAquinoSuzukiAinda não há avaliações
- Parasitology Revised SyllabusDocumento6 páginasParasitology Revised Syllabusshlmr_foxAinda não há avaliações
- Exercise 5 Hematocrit DeterminationDocumento7 páginasExercise 5 Hematocrit DeterminationJam RamosAinda não há avaliações
- MLS312 - Module04 - Explore - Experiment#6 - 0962 - Calpahi - Justine JadeDocumento4 páginasMLS312 - Module04 - Explore - Experiment#6 - 0962 - Calpahi - Justine JadeJustine Jade Atew CalpahiAinda não há avaliações
- AUBF Lecture Chemical Examination of UrineDocumento6 páginasAUBF Lecture Chemical Examination of UrineJane Yvette AndresAinda não há avaliações
- Case Study On LeukemiaDocumento55 páginasCase Study On LeukemialicservernoidaAinda não há avaliações
- Clinical Microscopy (Fecalysis)Documento2 páginasClinical Microscopy (Fecalysis)Sheng Ramos AglugubAinda não há avaliações
- Nature of the Clinical Laboratory T19Documento21 páginasNature of the Clinical Laboratory T19nicoAinda não há avaliações
- Final DX ResultsDocumento9 páginasFinal DX ResultszysheaiAinda não há avaliações
- CLS 400 - Test 4 (Extra Credit)Documento8 páginasCLS 400 - Test 4 (Extra Credit)McNeeseInsiderAinda não há avaliações
- CLS 400 - Anaerobes (Case Studies)Documento4 páginasCLS 400 - Anaerobes (Case Studies)McNeeseInsiderAinda não há avaliações
- Sample Questions For Emstrex 2012Documento6 páginasSample Questions For Emstrex 2012Dr.2020100% (1)
- L/L Research L/L Research: The TheDocumento16 páginasL/L Research L/L Research: The TheP D SpencerAinda não há avaliações
- L/L Research: The Aaron/Q'uo Dialogues, Session 3Documento8 páginasL/L Research: The Aaron/Q'uo Dialogues, Session 3P D SpencerAinda não há avaliações
- WeLearnAssessment FinalDocumento1 páginaWeLearnAssessment FinalP D SpencerAinda não há avaliações
- L/L Research L/L Research: The TheDocumento16 páginasL/L Research L/L Research: The TheP D SpencerAinda não há avaliações
- L/L Research: The Aaron/Q'uo Dialogues, Session 1Documento6 páginasL/L Research: The Aaron/Q'uo Dialogues, Session 1P D SpencerAinda não há avaliações
- Comp9 Unit2c Audio TranscriptDocumento4 páginasComp9 Unit2c Audio TranscriptP D SpencerAinda não há avaliações
- L/L Research: The Aaron/Q'uo Dialogues, Session 2Documento7 páginasL/L Research: The Aaron/Q'uo Dialogues, Session 2P D SpencerAinda não há avaliações
- MedtherpyDocumento2 páginasMedtherpyP D SpencerAinda não há avaliações
- L/L Research L/L Research: The TheDocumento16 páginasL/L Research L/L Research: The TheP D SpencerAinda não há avaliações
- Comp9 Unit3 Activities KeyDocumento1 páginaComp9 Unit3 Activities KeyP D SpencerAinda não há avaliações
- L/L Research L/L Research: The TheDocumento16 páginasL/L Research L/L Research: The TheP D SpencerAinda não há avaliações
- Comp 01 Instructor ManualDocumento54 páginasComp 01 Instructor ManualP D SpencerAinda não há avaliações
- Comp9 Unit3b Audio TranscriptDocumento13 páginasComp9 Unit3b Audio TranscriptP D SpencerAinda não há avaliações
- Comp9 Unit3a Audio TranscriptDocumento13 páginasComp9 Unit3a Audio TranscriptP D SpencerAinda não há avaliações
- Comp9 Unit3c Audio TranscriptDocumento9 páginasComp9 Unit3c Audio TranscriptP D SpencerAinda não há avaliações
- Comp9 Unit3 Self Assess KeyDocumento6 páginasComp9 Unit3 Self Assess KeyP D SpencerAinda não há avaliações
- Comp9 Unit4 Self AssessDocumento6 páginasComp9 Unit4 Self AssessP D SpencerAinda não há avaliações
- Comp9 Unit4 Self Assess KeyDocumento11 páginasComp9 Unit4 Self Assess KeyP D SpencerAinda não há avaliações
- Comp9 Unit3 ActivitiesDocumento1 páginaComp9 Unit3 ActivitiesP D SpencerAinda não há avaliações
- Comp9 Unit4 Activity KeyDocumento2 páginasComp9 Unit4 Activity KeyP D SpencerAinda não há avaliações
- Comp9 Unit3 Self AssessDocumento4 páginasComp9 Unit3 Self AssessP D SpencerAinda não há avaliações
- Comp9 Unit2b Audio TranscriptDocumento6 páginasComp9 Unit2b Audio TranscriptP D SpencerAinda não há avaliações
- Comp9 Unit5b Audio TranscriptDocumento12 páginasComp9 Unit5b Audio TranscriptP D SpencerAinda não há avaliações
- Comp9 Unit5c Audio TranscriptDocumento12 páginasComp9 Unit5c Audio TranscriptP D SpencerAinda não há avaliações
- Comp9 Unit4 ActivityDocumento1 páginaComp9 Unit4 ActivityP D SpencerAinda não há avaliações
- Comp9 Unit6 Activity KeyDocumento1 páginaComp9 Unit6 Activity KeyP D SpencerAinda não há avaliações
- Comp9 Unit6 Self AssessDocumento3 páginasComp9 Unit6 Self AssessP D SpencerAinda não há avaliações
- Comp9 Unit4e Audio TranscriptDocumento8 páginasComp9 Unit4e Audio TranscriptP D SpencerAinda não há avaliações
- Comp9 Unit5 Self AssessDocumento3 páginasComp9 Unit5 Self AssessP D SpencerAinda não há avaliações
- Comp9 Unit4a Audio TranscriptDocumento9 páginasComp9 Unit4a Audio TranscriptP D SpencerAinda não há avaliações
- @anesthesia Books 2016 PrinciplesDocumento372 páginas@anesthesia Books 2016 PrinciplesanayunitaAinda não há avaliações
- Techniques in AnesthesiaDocumento49 páginasTechniques in AnesthesiaGarry LasagaAinda não há avaliações
- Avenue Keeps On Living: Your Local NewsDocumento32 páginasAvenue Keeps On Living: Your Local NewsmooraboolAinda não há avaliações
- Sambong Health BenefitsDocumento2 páginasSambong Health BenefitsLyks YouAinda não há avaliações
- UTI Types, Symptoms, Diagnosis and TreatmentDocumento23 páginasUTI Types, Symptoms, Diagnosis and TreatmentShamila KaruthuAinda não há avaliações
- 1307 Ascot Bpla (Sever)Documento8 páginas1307 Ascot Bpla (Sever)Fernando CamargoAinda não há avaliações
- Poisonous PlantsDocumento12 páginasPoisonous Plantsriki187Ainda não há avaliações
- The Respiratory System PDFDocumento21 páginasThe Respiratory System PDFhechi_zeroAinda não há avaliações
- Poultry Production and Management PracticesDocumento126 páginasPoultry Production and Management Practicessamuel pineda100% (1)
- Child's Military Tuberculosis CaseDocumento31 páginasChild's Military Tuberculosis CaseRifka WindiputriAinda não há avaliações
- Genetic Basis of Inheritance: Types of Phenotypic TraitsDocumento16 páginasGenetic Basis of Inheritance: Types of Phenotypic TraitsknlsinhaAinda não há avaliações
- Nervous System WsDocumento11 páginasNervous System Wsapi-309893409Ainda não há avaliações
- Complete 9A PDFDocumento40 páginasComplete 9A PDFmillergra100% (1)
- Examination of Inguinoscrotal SwellingDocumento3 páginasExamination of Inguinoscrotal SwellingHumna YounisAinda não há avaliações
- Nutrition For The Denture PatientDocumento8 páginasNutrition For The Denture PatientKrupali JainAinda não há avaliações
- CWD Climax Surveillance FAQ FinalDocumento2 páginasCWD Climax Surveillance FAQ FinalinforumdocsAinda não há avaliações
- Agatha M. Thrash, M.D. Preventive Medicine DuringDocumento2 páginasAgatha M. Thrash, M.D. Preventive Medicine Duringapi-26198026Ainda não há avaliações
- Blood physiology components and functionsDocumento39 páginasBlood physiology components and functionsSarmad Laith MortadaAinda não há avaliações
- Lesley Ann Bergmeier (Eds.) - Oral Mucosa in Health and Disease - A Concise Handbook-Springer International Publishing (2018)Documento187 páginasLesley Ann Bergmeier (Eds.) - Oral Mucosa in Health and Disease - A Concise Handbook-Springer International Publishing (2018)Nadira Nurin100% (1)
- CamouflageDocumento172 páginasCamouflageAnonymous gUjimJKAinda não há avaliações
- Introduction To Nervous SystemDocumento69 páginasIntroduction To Nervous Systemadnan jan100% (1)
- Mechanisms of Bacterial PathogenesisDocumento34 páginasMechanisms of Bacterial PathogenesisMamta ShindeAinda não há avaliações
- CoccidiaDocumento42 páginasCoccidiawadige4668Ainda não há avaliações
- Viva Questions of Final Professional ExaminationDocumento48 páginasViva Questions of Final Professional ExaminationFaisol KabirAinda não há avaliações
- SKIN STRUCTURE &FUNCTION Lec 1Documento40 páginasSKIN STRUCTURE &FUNCTION Lec 1Sadia SohailAinda não há avaliações
- Essential Articles 12Documento208 páginasEssential Articles 12cencenhi100% (1)
- PZO9500EDocumento20 páginasPZO9500Estoryte11erAinda não há avaliações
- Excretory System WorksheetDocumento4 páginasExcretory System WorksheetMariela Belén RivasAinda não há avaliações
- Sci Quiz MusculoskeletalDocumento16 páginasSci Quiz MusculoskeletalJERVES FALCOTELOAinda não há avaliações
- OEC CH 18Documento10 páginasOEC CH 18Phil McLeanAinda não há avaliações