Você também pode gostar
- Lecture 2: The Boney Skeleton: Chapter 7 and 8Documento59 páginasLecture 2: The Boney Skeleton: Chapter 7 and 8lemonAinda não há avaliações
- OrthopaediDocumento87 páginasOrthopaediGalihAinda não há avaliações
- The Human SkeletonDocumento71 páginasThe Human Skeletontszkin13527Ainda não há avaliações
- Upper ExtremityDocumento15 páginasUpper ExtremityLomongo ChristianAinda não há avaliações
- Bedah 2 Batch 3 2018Documento87 páginasBedah 2 Batch 3 2018Meiza Ihsan FakhriAinda não há avaliações
- Orthopedic FinalDocumento858 páginasOrthopedic Finalhashmf180% (10)
- Lecture 9 Emergency ProceduresDocumento59 páginasLecture 9 Emergency ProceduresAniqa AsgharAinda não há avaliações
- Cervical Spine Proto GihDocumento8 páginasCervical Spine Proto GihAndy Delos ReyesAinda não há avaliações
- 16 Upper Extremity (FINAL)Documento30 páginas16 Upper Extremity (FINAL)kath-kath100% (1)
- Thorax 1Documento109 páginasThorax 1Insyirah JohariAinda não há avaliações
- L2 Joints of Axial Appendicular Skeleton - 2020-2021 - CompressedDocumento12 páginasL2 Joints of Axial Appendicular Skeleton - 2020-2021 - CompressedARYSSA BINTI AZRIAinda não há avaliações
- 2 System Musculo Sceletal 2014Documento41 páginas2 System Musculo Sceletal 2014leni sharaAinda não há avaliações
- 09:16 - Back & Spinal Cord PDFDocumento24 páginas09:16 - Back & Spinal Cord PDFVidya BalaAinda não há avaliações
- Back Spine AnatomyDocumento3 páginasBack Spine AnatomyNinjaAinda não há avaliações
- Back - Spine (Chapter 12)Documento9 páginasBack - Spine (Chapter 12)Alenna BenitezAinda não há avaliações
- (Mantap) Slide Materi Bedah-2 Batch 3 2018 SalinanDocumento200 páginas(Mantap) Slide Materi Bedah-2 Batch 3 2018 SalinantikaAinda não há avaliações
- Lab 2 SlidesDocumento10 páginasLab 2 SlidesMikeAinda não há avaliações
- 1 - The SkullDocumento68 páginas1 - The Skullaboody omerAinda não há avaliações
- LE Conditions PASTDocumento10 páginasLE Conditions PASTGelo BombitzAinda não há avaliações
- Bimbingan Muskuloskeletal CoassDocumento224 páginasBimbingan Muskuloskeletal CoassMichael AndhitoAinda não há avaliações
- Anatomy and Physiology 6th Edition Marieb Solutions Manual Full Chapter PDFDocumento41 páginasAnatomy and Physiology 6th Edition Marieb Solutions Manual Full Chapter PDFserenafinnodx100% (10)
- Anatomy and Physiology 6th Edition Marieb Solutions ManualDocumento20 páginasAnatomy and Physiology 6th Edition Marieb Solutions Manualstephenthanh1huo100% (28)
- Anatomical TerminologyDocumento57 páginasAnatomical TerminologyAlicina DaleAinda não há avaliações
- Reviewer GHSB - Prelims PDFDocumento4 páginasReviewer GHSB - Prelims PDFTj AgudillaAinda não há avaliações
- Bones of Upper and Lower Limbs - RevisionDocumento15 páginasBones of Upper and Lower Limbs - RevisionChess Nuts100% (1)
- Bedah 2: Bedah Orthopaedi, Urologi, Digestive, Onkologi Batch Agustus 2018 ContributorDocumento200 páginasBedah 2: Bedah Orthopaedi, Urologi, Digestive, Onkologi Batch Agustus 2018 ContributorGalihAinda não há avaliações
- Anatomy From The DoctorDocumento208 páginasAnatomy From The DoctorSweet manAinda não há avaliações
- Head Neck TMJDocumento4 páginasHead Neck TMJNinjaAinda não há avaliações
- SkullDocumento57 páginasSkullCharmaine LucAinda não há avaliações
- Midfi Patho 2Documento8 páginasMidfi Patho 2Rachelle Danya Dela RosaAinda não há avaliações
- Basic Radiology PDFDocumento104 páginasBasic Radiology PDFsimona mariana dutu100% (1)
- Summary MRI Knee ImagingDocumento17 páginasSummary MRI Knee ImagingSoban DaudAinda não há avaliações
- Anatomy of Spine: DR Pankaj N Surange MBBS, MD, Fipp Interventional Pain and Spine SpecialistDocumento72 páginasAnatomy of Spine: DR Pankaj N Surange MBBS, MD, Fipp Interventional Pain and Spine SpecialistMohammad Riedho Cahya AtazsuAinda não há avaliações
- Chapter 6. Axial Skeleton: I. Radiographic AnatomyDocumento11 páginasChapter 6. Axial Skeleton: I. Radiographic AnatomyRindha Dwi SihantoAinda não há avaliações
- Orthopaedics OsceDocumento39 páginasOrthopaedics OsceLana Loco50% (2)
- Orbit - Head & NeckDocumento57 páginasOrbit - Head & NeckNandini BhargavaAinda não há avaliações
- Joints and Ligaments of The Skull and Neck-2Documento79 páginasJoints and Ligaments of The Skull and Neck-2armanious64Ainda não há avaliações
- DR Tourkey Note New Edition MRCSDocumento468 páginasDR Tourkey Note New Edition MRCSchenghui maAinda não há avaliações
- Axial Anatomy: AY 2019-2020 Dr. Paredes Aug. 27, 2019Documento11 páginasAxial Anatomy: AY 2019-2020 Dr. Paredes Aug. 27, 2019Jose Emmanuel DolorAinda não há avaliações
- Ther150 Week 2 1 StudentDocumento27 páginasTher150 Week 2 1 StudentKaashvi GuptaAinda não há avaliações
- 21 Prosthetics (FINAL)Documento7 páginas21 Prosthetics (FINAL)kath-kathAinda não há avaliações
- Anaphy Midterm Reviewer1Documento14 páginasAnaphy Midterm Reviewer1juddee.conejosAinda não há avaliações
- Chinchilla SkullDocumento12 páginasChinchilla Skullf.baobao28Ainda não há avaliações
- GFHDocumento34 páginasGFHaisa mutiaraAinda não há avaliações
- Orthopedic Surgery NotesDocumento3 páginasOrthopedic Surgery NotesJoel Salu100% (1)
- Neurologic Conditions 1 SciDocumento5 páginasNeurologic Conditions 1 SciEdward De LeonAinda não há avaliações
- 4-Fracture 2 FDocumento30 páginas4-Fracture 2 FRadwa TalaatAinda não há avaliações
- ABC Imaging 1 - The SpineDocumento145 páginasABC Imaging 1 - The SpineAna-Maria PaunescuAinda não há avaliações
- Radio Lec 04 MusculoskeletalDocumento4 páginasRadio Lec 04 Musculoskeletalapi-3704562Ainda não há avaliações
- A2-ATM Cursul 2Documento9 páginasA2-ATM Cursul 2stefania georgescuAinda não há avaliações
- Spine X Ray Final May 2023Documento64 páginasSpine X Ray Final May 2023sayedoooovAinda não há avaliações
- BMED - Lecture 7 PDFDocumento5 páginasBMED - Lecture 7 PDFDaniella Stevanato SanchezAinda não há avaliações
- Anatomy of Cervical SpineDocumento29 páginasAnatomy of Cervical SpineManiAinda não há avaliações
- Cervical X-RayDocumento8 páginasCervical X-RayRio Yus RamadhaniAinda não há avaliações
- Skull: Handout VersionDocumento57 páginasSkull: Handout VersionTdoc TonyAinda não há avaliações
- HA L2 Assessing Head, Neck, Breasts, and Lymphatic SystemDocumento3 páginasHA L2 Assessing Head, Neck, Breasts, and Lymphatic SystemljtorreslriejyAinda não há avaliações
- 1-1 Anatomie Des Extenseurs Des Doigts LongsDocumento20 páginas1-1 Anatomie Des Extenseurs Des Doigts LongsProfesseur Christian DumontierAinda não há avaliações
- Neck Stability: A Lecture by J. Douglas-Morris ForDocumento16 páginasNeck Stability: A Lecture by J. Douglas-Morris ForJoseph LeeAinda não há avaliações
- Module 14 Pediatric TB ENGLISHDocumento85 páginasModule 14 Pediatric TB ENGLISHDellAinda não há avaliações
- Jurnal Farmakologi Anti Konvulsi PDFDocumento13 páginasJurnal Farmakologi Anti Konvulsi PDFtherempongss100% (1)
- Family Planning HandbookDocumento387 páginasFamily Planning HandbookvthiseasAinda não há avaliações
- 5 Morisky Medication Adherence-Scale PDFDocumento1 página5 Morisky Medication Adherence-Scale PDFDellAinda não há avaliações
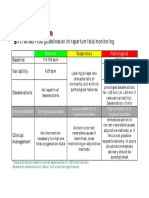
- CTG Classification PDFDocumento1 páginaCTG Classification PDFDellAinda não há avaliações
- A Practical Classification of Septonasal Deviation.42Documento3 páginasA Practical Classification of Septonasal Deviation.42DellAinda não há avaliações
- SPSS Crosstab PDFDocumento3 páginasSPSS Crosstab PDFDellAinda não há avaliações
- Cutaneous Tuberculosis: Epidemiologic, Etiopathogenic and Clinical Aspects - Part IDocumento10 páginasCutaneous Tuberculosis: Epidemiologic, Etiopathogenic and Clinical Aspects - Part IDellAinda não há avaliações
- 5 Morisky Medication Adherence-Scale PDFDocumento1 página5 Morisky Medication Adherence-Scale PDFDellAinda não há avaliações
- Fitzpatrick's Dermatology in General Medicine, Eighth Edition, 2 Volume SetDocumento30 páginasFitzpatrick's Dermatology in General Medicine, Eighth Edition, 2 Volume SetDellAinda não há avaliações
- Appendix 8 Normal Urine Output PDFDocumento1 páginaAppendix 8 Normal Urine Output PDFDellAinda não há avaliações
- Extraction of Wisdom Teeth Under General Anesthesia-A StudyDocumento5 páginasExtraction of Wisdom Teeth Under General Anesthesia-A StudyCiutac ŞtefanAinda não há avaliações
- Respiratory Emergencies in ChildrenDocumento66 páginasRespiratory Emergencies in Childrenlordoftheweb100% (7)
- 5.PHC 24 X 7 5th Jan 11Documento12 páginas5.PHC 24 X 7 5th Jan 11National Child Health Resource Centre (NCHRC)Ainda não há avaliações
- Benign Paroxysmal Positional Vertigo Pathophysiology, Causes, Canal Variants and Treatment PDFDocumento8 páginasBenign Paroxysmal Positional Vertigo Pathophysiology, Causes, Canal Variants and Treatment PDFegyzellahsAinda não há avaliações
- Tracheoesophageal FistulaDocumento6 páginasTracheoesophageal FistulaPankaj SinghAinda não há avaliações
- 000 MOI-AtlantaDocumento63 páginas000 MOI-AtlantajoandersontiagoAinda não há avaliações
- Persistent Pulmonary Hypertension of The NewbornDocumento4 páginasPersistent Pulmonary Hypertension of The NewbornMarwa Adly100% (1)
- Evaluation of A Tracheostomy Education Programme For Speech-Language TherapistsDocumento15 páginasEvaluation of A Tracheostomy Education Programme For Speech-Language TherapistsmochkurniawanAinda não há avaliações
- (HeartSim 200 DfU) - 982Documento86 páginas(HeartSim 200 DfU) - 982edgargadoAinda não há avaliações
- Neonatal Jaundice CME ANisDocumento47 páginasNeonatal Jaundice CME ANisAnisAinda não há avaliações
- Pulmonary Auscultation PDFDocumento5 páginasPulmonary Auscultation PDFThatikala AbhilashAinda não há avaliações
- WarmTouch VETDocumento8 páginasWarmTouch VETBertha DuránAinda não há avaliações
- What Is An Office Hysteroscopy?Documento4 páginasWhat Is An Office Hysteroscopy?ericAinda não há avaliações
- Public Hearing Proposed Classification Hospitals and Other Health Facilities 2mar2012 DuqueHall Post DOHWebsiteDocumento24 páginasPublic Hearing Proposed Classification Hospitals and Other Health Facilities 2mar2012 DuqueHall Post DOHWebsiteHarby Ongbay AbellanosaAinda não há avaliações
- Kaplan Peds ConceptsDocumento8 páginasKaplan Peds ConceptsnanaAinda não há avaliações
- Phototherapy ChecklistDocumento2 páginasPhototherapy ChecklistMA. JIZELLE (CELSO) SINFUEGO100% (2)
- Neonate TransferDocumento4 páginasNeonate TransferDelphy VargheseAinda não há avaliações
- Qa Tables FinalDocumento11 páginasQa Tables Finalapi-337188982Ainda não há avaliações
- Cataract Aiims Aipgmee Pgi Jipmer DNB McqsDocumento41 páginasCataract Aiims Aipgmee Pgi Jipmer DNB Mcqsजेनिश न्यौपानेAinda não há avaliações
- Bosentan PI PDFDocumento12 páginasBosentan PI PDFlaghatechinmayAinda não há avaliações
- Mesiodens Etiology, Prevalence, Diagnosis and ManagementDocumento4 páginasMesiodens Etiology, Prevalence, Diagnosis and ManagementsyedAinda não há avaliações
- Anatomy MCQDocumento23 páginasAnatomy MCQPirabakar Mahendran100% (3)
- Apocrine Breast LesionsDocumento7 páginasApocrine Breast LesionscandiddreamsAinda não há avaliações
- Health TC Notes, DMHO and DCHS Reports 03-09-2022, 6AMDocumento14 páginasHealth TC Notes, DMHO and DCHS Reports 03-09-2022, 6AMPraneeth TsavatapalliAinda não há avaliações
- ALGA Medical NetworkDocumento56 páginasALGA Medical NetworkCarl HernandezAinda não há avaliações
- Basal Cell Carcinoma: CausesDocumento5 páginasBasal Cell Carcinoma: CausesRini LianingsihAinda não há avaliações
- HEENT History TakingDocumento15 páginasHEENT History TakingPépé TechopathamAinda não há avaliações
- Mandibular Overdenture PDFDocumento103 páginasMandibular Overdenture PDFIbrahim Ahmed Dahab100% (1)
- A Proven Pathway To AccreditationDocumento25 páginasA Proven Pathway To AccreditationkukunAinda não há avaliações
- Indexed Journals of Pakistan - Medline and EmbaseDocumento48 páginasIndexed Journals of Pakistan - Medline and EmbaseFaisal RoohiAinda não há avaliações