Você também pode gostar
- Carbohydrate and Fat Utilization During Rest and Physical ActivityDocumento8 páginasCarbohydrate and Fat Utilization During Rest and Physical ActivitySyifa Choerunisa AisyahAinda não há avaliações
- Nutrition For Sport and Exercise 3rd Edition Dunford Doyle 128575249X Solution ManualDocumento12 páginasNutrition For Sport and Exercise 3rd Edition Dunford Doyle 128575249X Solution Manuallouise100% (28)
- Solution Manual For Nutrition For Sport and Exercise 3Rd Edition Dunford Doyle 128575249X 9781285752495 Full Chapter PDFDocumento33 páginasSolution Manual For Nutrition For Sport and Exercise 3Rd Edition Dunford Doyle 128575249X 9781285752495 Full Chapter PDFmary.cannon812100% (15)
- Dwnload Full Nutrition For Sport and Exercise 3rd Edition Dunford Solutions Manual PDFDocumento35 páginasDwnload Full Nutrition For Sport and Exercise 3rd Edition Dunford Solutions Manual PDFsoeungsitterx100% (9)
- Full Download Nutrition For Sport and Exercise 3rd Edition Dunford Solutions ManualDocumento35 páginasFull Download Nutrition For Sport and Exercise 3rd Edition Dunford Solutions Manualkeathleyjessiavipfx100% (38)
- Energy Expenditure and FatigueDocumento49 páginasEnergy Expenditure and FatigueAh Zhang100% (1)
- Work, Energy, and Power in Humans: PhysicsDocumento14 páginasWork, Energy, and Power in Humans: PhysicsAbeer FatimaAinda não há avaliações
- Nutrition For Sport and Exercise 3rd Edition Dunford Solutions ManualDocumento11 páginasNutrition For Sport and Exercise 3rd Edition Dunford Solutions Manuala731535732Ainda não há avaliações
- Chapter 3 - Measurement of Physical Activity - EJFDocumento33 páginasChapter 3 - Measurement of Physical Activity - EJFVonderAinda não há avaliações
- XXII. Measurement of Basal Metabolic Expenditure (BME) Using Indirect Calorimetry XXIII. Calculation of Energy ExpenditureDocumento11 páginasXXII. Measurement of Basal Metabolic Expenditure (BME) Using Indirect Calorimetry XXIII. Calculation of Energy ExpenditureTaha OjisanAinda não há avaliações
- The EndDocumento25 páginasThe Endinfobusiness2010Ainda não há avaliações
- Energy Systems To Power The AthleteDocumento34 páginasEnergy Systems To Power The Athletemahnoor fatimaAinda não há avaliações
- CV Adaptations, HIIT, FatigueDocumento3 páginasCV Adaptations, HIIT, FatigueTamas KalmarAinda não há avaliações
- Metabolic RateDocumento10 páginasMetabolic RateABAYNEGETAHUN getahunAinda não há avaliações
- Brooks - ch04 BASICS OF METABOLISMDocumento16 páginasBrooks - ch04 BASICS OF METABOLISMSergio Andres Chacon PedrazaAinda não há avaliações
- Practice 3Documento7 páginasPractice 3Iryna ShpakAinda não há avaliações
- BBT423 L2Documento23 páginasBBT423 L2wowipev155Ainda não há avaliações
- Metabolism LabDocumento3 páginasMetabolism LabJerry SmithAinda não há avaliações
- Medical Physics: Energy, Work and Power of TheDocumento10 páginasMedical Physics: Energy, Work and Power of TheMarci MunirAinda não há avaliações
- Cho2016 ADocumento4 páginasCho2016 AJuan Pablo Espinoza PuellesAinda não há avaliações
- Physiology Lab Report Title of Report: Cardiorespiratory Effects of ExerciseDocumento9 páginasPhysiology Lab Report Title of Report: Cardiorespiratory Effects of ExerciseKogo VickAinda não há avaliações
- Metabolism 1 1819Documento28 páginasMetabolism 1 1819Liaqat HussainAinda não há avaliações
- Measurement of Work, Power, and Energy Expenditure: Prepared By: Sonya Arshad B.SC Hons, M.SC, B.Ed, MphillDocumento40 páginasMeasurement of Work, Power, and Energy Expenditure: Prepared By: Sonya Arshad B.SC Hons, M.SC, B.Ed, MphillUzairAinda não há avaliações
- Ê V Ê Ê V Ê V Ê V Ê V Ê V Ê V ÊDocumento5 páginasÊ V Ê Ê V Ê V Ê V Ê V Ê V Ê V ÊscribdmelwinAinda não há avaliações
- When Somebody Loses Weight, Where Does The Fat Go ?Documento3 páginasWhen Somebody Loses Weight, Where Does The Fat Go ?Sílfide Xanat100% (1)
- Monitoring of Bioimpedance Data During Exercise in CyclistsDocumento6 páginasMonitoring of Bioimpedance Data During Exercise in CyclistsgvozdenAinda não há avaliações
- Exercise Physiology: Dr. Adelia Handoko, M.SiDocumento92 páginasExercise Physiology: Dr. Adelia Handoko, M.SiAdel Lia100% (2)
- Class Note NUT 301 - 3 - ENERGY REQUIREMENTSDocumento13 páginasClass Note NUT 301 - 3 - ENERGY REQUIREMENTSomonzejele jenniferAinda não há avaliações
- Cellular Respiration LabDocumento6 páginasCellular Respiration Labianzhou1Ainda não há avaliações
- HargreavesSpriet-2020 Skeletal Muscle Energy Metabolism Duringa ExerciseDocumento13 páginasHargreavesSpriet-2020 Skeletal Muscle Energy Metabolism Duringa ExerciseBRUNA MARIA PEREIRA DA SILVAAinda não há avaliações
- Human NutritionDocumento33 páginasHuman NutritionPravin BabareAinda não há avaliações
- Aerobic Exercises 2Documento71 páginasAerobic Exercises 2Jen Passilan100% (1)
- Metabolic Calculations ACSM PowePointDocumento9 páginasMetabolic Calculations ACSM PowePointKatoAinda não há avaliações
- Aerobic Exercise 1Documento73 páginasAerobic Exercise 1Badahdah , Omar Abdulaziz SaeedAinda não há avaliações
- Excess Post-Exercise Oxygen Consumption: 2 Size of The EPOC EffectDocumento3 páginasExcess Post-Exercise Oxygen Consumption: 2 Size of The EPOC EffectFAZRI MOAinda não há avaliações
- Macronutrients NSCADocumento3 páginasMacronutrients NSCAEmanuele DanieleAinda não há avaliações
- Intermittent Resistance Exercise: Evolution From The Steady StateDocumento8 páginasIntermittent Resistance Exercise: Evolution From The Steady StatejuanAinda não há avaliações
- Prinsip Bioenergitika Dan Metabolisme Olahraga - Prof. YusniDocumento68 páginasPrinsip Bioenergitika Dan Metabolisme Olahraga - Prof. YusniArolAinda não há avaliações
- When Somebody Loses Weight, Where Does The Fat GoDocumento3 páginasWhen Somebody Loses Weight, Where Does The Fat GoEdsonAinda não há avaliações
- Metabolism of Carbohydrate: Department of Biochemistry Faculty of Medicine University of YARSI JakartaDocumento60 páginasMetabolism of Carbohydrate: Department of Biochemistry Faculty of Medicine University of YARSI JakartaAmanda PutriAinda não há avaliações
- UT Dallas Syllabus For Biol3370.001.11s Taught by Irina Borovkov (Ixb053000)Documento4 páginasUT Dallas Syllabus For Biol3370.001.11s Taught by Irina Borovkov (Ixb053000)UT Dallas Provost's Technology GroupAinda não há avaliações
- Foodworks AssignmentDocumento3 páginasFoodworks AssignmentYoussef LatashAinda não há avaliações
- Challenges in Tackling Energy Expenditure As Obesity Therapy: From Preclinical Models To Clinical ApplicationDocumento15 páginasChallenges in Tackling Energy Expenditure As Obesity Therapy: From Preclinical Models To Clinical ApplicationHadrien DemagnyAinda não há avaliações
- Metabolism and Energy BalanceDocumento49 páginasMetabolism and Energy BalanceMadya Pratama100% (1)
- Bio5 LabManual F19 1.0Documento138 páginasBio5 LabManual F19 1.0Catherine BrennanAinda não há avaliações
- Exercise Physiology Course NotesDocumento131 páginasExercise Physiology Course NotesAdam Linoby100% (16)
- The Physiology of Cell Energy Production: CPTIPS.COM MonographsNo EverandThe Physiology of Cell Energy Production: CPTIPS.COM MonographsAinda não há avaliações
- Nikhil BTP Mid Term ReportDocumento17 páginasNikhil BTP Mid Term ReportNikhil SaiyamAinda não há avaliações
- Metabolism 1112 PracticalDocumento39 páginasMetabolism 1112 PracticalKamran AfzalAinda não há avaliações
- Nutrition - Energy ValueDocumento8 páginasNutrition - Energy ValueSubhashini WilliamsAinda não há avaliações
- When Somebody Loses Weight, Where Does The Fat GoDocumento3 páginasWhen Somebody Loses Weight, Where Does The Fat Gopruebas123123Ainda não há avaliações
- When Somebody Loses Weight, WHDocumento3 páginasWhen Somebody Loses Weight, WHopus57Ainda não há avaliações
- Lab 4 - Aerobic Energy Expenditure 1 - WebsiteDocumento10 páginasLab 4 - Aerobic Energy Expenditure 1 - Websiteapi-708484558Ainda não há avaliações
- Exercise Physiology Syllabus PDFDocumento13 páginasExercise Physiology Syllabus PDFAsif ZubairAinda não há avaliações
- Gen Bio. 2ND Quarter RespirationDocumento3 páginasGen Bio. 2ND Quarter RespirationChrislyn Eds Javier AcobAinda não há avaliações
- Huma Body Thermal AnalysisDocumento5 páginasHuma Body Thermal Analysisrajeesh radhakrishnanAinda não há avaliações
- Bishop 2010Documento9 páginasBishop 2010Marcos CavalcanteAinda não há avaliações
- Clin AcsmDocumento2 páginasClin AcsmArmando Alves de MatosAinda não há avaliações
- Summary of Steve House, Scott Johnston & Kilian Jornet's Training for the Uphill AthleteNo EverandSummary of Steve House, Scott Johnston & Kilian Jornet's Training for the Uphill AthleteAinda não há avaliações
- 17 - Enhanced Recovery PrinciplesDocumento7 páginas17 - Enhanced Recovery Principlesbocah_britpopAinda não há avaliações
- 08 - Oral and Sip FeedingDocumento11 páginas08 - Oral and Sip Feedingbocah_britpopAinda não há avaliações
- 17 - The Traumatized PatientDocumento7 páginas17 - The Traumatized Patientbocah_britpopAinda não há avaliações
- 03 - Nutritional Screening and Assessment PDFDocumento8 páginas03 - Nutritional Screening and Assessment PDFbocah_britpop100% (1)
- 08 - Indications, Contraindications, Complications and Monitoring of enDocumento13 páginas08 - Indications, Contraindications, Complications and Monitoring of enbocah_britpopAinda não há avaliações
- ACS SabistonDocumento10 páginasACS Sabistonbocah_britpopAinda não há avaliações
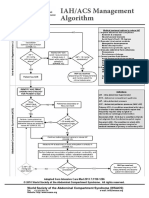
- IAH ACS Medical Management 2014Documento1 páginaIAH ACS Medical Management 2014bocah_britpopAinda não há avaliações
- Intraabdominal Pressure MonitoringDocumento10 páginasIntraabdominal Pressure Monitoringbocah_britpopAinda não há avaliações
- Case Disc RadioDocumento29 páginasCase Disc Radiobocah_britpopAinda não há avaliações
- IAH ACS Management 2014Documento1 páginaIAH ACS Management 2014bocah_britpopAinda não há avaliações
- Tuesday, March 09 2015: Team in ChargeDocumento2 páginasTuesday, March 09 2015: Team in Chargebocah_britpopAinda não há avaliações
- Femur Fractures in Infants and Young ChildrenDocumento3 páginasFemur Fractures in Infants and Young Childrenbocah_britpopAinda não há avaliações
- Tuesday, March 09 2015: Team in ChargeDocumento7 páginasTuesday, March 09 2015: Team in Chargebocah_britpopAinda não há avaliações
- Art 3A10.1007 2Fs11832 014 0590 3Documento7 páginasArt 3A10.1007 2Fs11832 014 0590 3bocah_britpopAinda não há avaliações
- University of Colorado NICHE Practice Survey SummaryDocumento48 páginasUniversity of Colorado NICHE Practice Survey Summarybocah_britpopAinda não há avaliações
- Femur Fractures in The Pediatric Population: Abuse or Accidental Trauma?Documento7 páginasFemur Fractures in The Pediatric Population: Abuse or Accidental Trauma?bocah_britpopAinda não há avaliações
- Spectrum of Operative Childhood Intra-Articular Shoulder PathologyDocumento4 páginasSpectrum of Operative Childhood Intra-Articular Shoulder Pathologybocah_britpopAinda não há avaliações
- Pediatrics 2010 Ravichandiran 60 6Documento9 páginasPediatrics 2010 Ravichandiran 60 6bocah_britpopAinda não há avaliações
- Laporan Alam Sekitar-JAS 2020Documento180 páginasLaporan Alam Sekitar-JAS 2020hazirulAinda não há avaliações
- Smoking Cheat SheetDocumento8 páginasSmoking Cheat SheetMyra BuellaAinda não há avaliações
- Sleep Disorders: Types & TreatmentsDocumento32 páginasSleep Disorders: Types & TreatmentsDM AfteniAinda não há avaliações
- Rev Med Chile 1997 Vol 125 (12) 1429-1436 1 EMBARAZO PDFDocumento8 páginasRev Med Chile 1997 Vol 125 (12) 1429-1436 1 EMBARAZO PDFSaraMarmolejoAinda não há avaliações
- Lesson 2Documento53 páginasLesson 2Courtney BurkinAinda não há avaliações
- Upaya Penurunan Stunting Melalui Suplemen GiziDocumento55 páginasUpaya Penurunan Stunting Melalui Suplemen GiziSubadi SubadiAinda não há avaliações
- Classification Essay SampleDocumento3 páginasClassification Essay SampleAlvin Malquisto100% (2)
- Pengaruh Penerapan Carbohydrate Loading Modifikasi Terhadap Kesegaran Jasmani Atlet Sepak BolaDocumento13 páginasPengaruh Penerapan Carbohydrate Loading Modifikasi Terhadap Kesegaran Jasmani Atlet Sepak BolaRizqiAnnisaPermatasariAinda não há avaliações
- 7 Different Exercises: Stretching Before WorkoutDocumento5 páginas7 Different Exercises: Stretching Before Workoutcly espinosaAinda não há avaliações
- Merrell Dow Pharmaceutical Meeting 1982Documento1 páginaMerrell Dow Pharmaceutical Meeting 1982Julia PurperaAinda não há avaliações
- Learning Materials in PE 1 LMs 4 6Documento29 páginasLearning Materials in PE 1 LMs 4 6Athena GwenAinda não há avaliações
- HDHK 1Documento26 páginasHDHK 1swaftyAinda não há avaliações
- Dance Is Another Form of Exercising Which Require You To Use Most of Your Body MuscleDocumento1 páginaDance Is Another Form of Exercising Which Require You To Use Most of Your Body MuscleEmily BrowneAinda não há avaliações
- Tobacco Lesson PlanDocumento4 páginasTobacco Lesson Planapi-240857737Ainda não há avaliações
- Health - : DieteticsDocumento3 páginasHealth - : DieteticsApple BananaAinda não há avaliações
- Air Pollution Control, A Design ApproachDocumento427 páginasAir Pollution Control, A Design ApproachMahmoud Basha95% (96)
- 4 Materi - DR Khayan PDFDocumento13 páginas4 Materi - DR Khayan PDFAfif BarcaAinda não há avaliações
- The ShredSmart Program - Third Edition Free Sample PDFDocumento32 páginasThe ShredSmart Program - Third Edition Free Sample PDFMiheer SinghAinda não há avaliações
- Nutrition 101Documento7 páginasNutrition 101api-168454738Ainda não há avaliações
- Custom Keto Meal Plan Email SequenceDocumento19 páginasCustom Keto Meal Plan Email SequenceKa R NaAinda não há avaliações
- Score Per Subject MendelDocumento36 páginasScore Per Subject MendelEdimar RingorAinda não há avaliações
- Joyner 1991Documento5 páginasJoyner 1991Gust AvoAinda não há avaliações
- Tentatif Latihan:: FASA 1 (SESI PAGI) 8.00AM - 9.30AM (Selasa, Rabu, Khamis)Documento1 páginaTentatif Latihan:: FASA 1 (SESI PAGI) 8.00AM - 9.30AM (Selasa, Rabu, Khamis)Kang Lip WeeAinda não há avaliações
- Sf8 Nutritional Status Grade 3 Del PilarDocumento8 páginasSf8 Nutritional Status Grade 3 Del PilarYesha Lucas AcuñaAinda não há avaliações
- Quiz On Physical Fitess TestDocumento4 páginasQuiz On Physical Fitess TestAbs TroyAinda não há avaliações
- Nutrition AssignmentDocumento10 páginasNutrition AssignmentAhmd MaxydAinda não há avaliações
- Final EssayDocumento12 páginasFinal EssayKayla RuppAinda não há avaliações
- How To Create A Strength Training ProgramDocumento6 páginasHow To Create A Strength Training ProgramWes Geary100% (1)
- Amplify: Workout Plan Designed by DR Jinger GottschallDocumento4 páginasAmplify: Workout Plan Designed by DR Jinger GottschallAlexis TrujilloAinda não há avaliações
- HSE Policy TemplateDocumento2 páginasHSE Policy Templateawong_911374Ainda não há avaliações