Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Juris Chapter 9Documento4 páginasJuris Chapter 9IS99057Ainda não há avaliações
- Congenital Heart DiseaseDocumento93 páginasCongenital Heart DiseaseManjunatha HR100% (1)
- 7 Types of ADHD PDFDocumento3 páginas7 Types of ADHD PDFAamir Malik67% (3)
- Home Care: Fatima University Medical Center FMCH DepartmentDocumento19 páginasHome Care: Fatima University Medical Center FMCH DepartmentIS99057100% (1)
- Anti Thrombotic Drugs and Transfusion MedicineDocumento5 páginasAnti Thrombotic Drugs and Transfusion MedicineIS99057Ainda não há avaliações
- Hematology: Benign White Cell Disorder DR Thuy Feb 21 2017Documento5 páginasHematology: Benign White Cell Disorder DR Thuy Feb 21 2017IS99057Ainda não há avaliações
- BronchiectasisDocumento9 páginasBronchiectasisIS99057Ainda não há avaliações
- Coagulation DisordersDocumento9 páginasCoagulation DisordersIS99057Ainda não há avaliações
- Psychopharmacology: Rainier B. Umali, M.DDocumento198 páginasPsychopharmacology: Rainier B. Umali, M.DIS99057Ainda não há avaliações
- Dopamine Receptor AntagonistsDocumento25 páginasDopamine Receptor AntagonistsIS99057Ainda não há avaliações
- Observational: Observing Participants. You CannotDocumento6 páginasObservational: Observing Participants. You CannotIS99057Ainda não há avaliações
- Epidemiologic Studies TransDocumento5 páginasEpidemiologic Studies TransIS99057Ainda não há avaliações
- Appnut Finals (No Aging)Documento12 páginasAppnut Finals (No Aging)IS99057Ainda não há avaliações
- Neoplasia I - RecordingDocumento6 páginasNeoplasia I - RecordingIS99057Ainda não há avaliações
- Orthotics and Assistive Devices OrthoticsDocumento3 páginasOrthotics and Assistive Devices OrthoticsIS99057Ainda não há avaliações
- Pigments (Residual Autophagic Bodies)Documento2 páginasPigments (Residual Autophagic Bodies)IS99057Ainda não há avaliações
- Legal Med - Ratio CompleteDocumento25 páginasLegal Med - Ratio CompleteIS99057Ainda não há avaliações
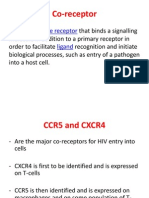
- Co-Receptor: Cell Surface Receptor LigandDocumento11 páginasCo-Receptor: Cell Surface Receptor LigandIS99057Ainda não há avaliações
- NCM 107 BDocumento3 páginasNCM 107 BGelain Joyce OrculloAinda não há avaliações
- Orthoheal - DNB Ortho Theory Question Papers AnalysisDocumento29 páginasOrthoheal - DNB Ortho Theory Question Papers AnalysisSivaprasath JaganathanAinda não há avaliações
- Energy Medicine For TodayDocumento31 páginasEnergy Medicine For TodayIvan VassilevAinda não há avaliações
- Ethico Moral Aspects of Nursing 2018Documento50 páginasEthico Moral Aspects of Nursing 2018Zyla De SagunAinda não há avaliações
- Form A: Use This Form For Initial Physical ExamDocumento4 páginasForm A: Use This Form For Initial Physical ExamLisa WillardsonAinda não há avaliações
- Morgan Mikhails Clinical Anesthesiology 6th Ed 2018 (2018-2114)Documento97 páginasMorgan Mikhails Clinical Anesthesiology 6th Ed 2018 (2018-2114)Wiwik SundariAinda não há avaliações
- Case StudyDocumento27 páginasCase Studyapi-313356122Ainda não há avaliações
- OcclusionDocumento49 páginasOcclusionRajsandeep SinghAinda não há avaliações
- 6.Intra-Arch DistractionDocumento15 páginas6.Intra-Arch DistractionMónica C. BadilloAinda não há avaliações
- 2009 Final Program PAAO PapersDocumento16 páginas2009 Final Program PAAO PapersMonica MendozaAinda não há avaliações
- Nursing Specialties Entre in Nursing//midtermDocumento4 páginasNursing Specialties Entre in Nursing//midtermfatty jaiAinda não há avaliações
- United Biotech WorldDocumento9 páginasUnited Biotech Worldswtyneha33Ainda não há avaliações
- Cervicogenic Dizziness: DefinitionDocumento9 páginasCervicogenic Dizziness: DefinitionpervinkumarAinda não há avaliações
- Framework For Maternal and Child Health NursingDocumento3 páginasFramework For Maternal and Child Health NursingRevex OcampoAinda não há avaliações
- 3-MedicalWriting IMRADManuscriptStructure PDFDocumento45 páginas3-MedicalWriting IMRADManuscriptStructure PDFJohn Dave MarbellaAinda não há avaliações
- Coleen Faye Molina Rubio. Cachola Jr. RNDocumento2 páginasColeen Faye Molina Rubio. Cachola Jr. RNdhandah100% (4)
- Classic Pulse Diagnosis PDFDocumento21 páginasClassic Pulse Diagnosis PDFDani TenaAinda não há avaliações
- Guidelines Develeopment Skills Labs MedicalCollegesDocumento2 páginasGuidelines Develeopment Skills Labs MedicalCollegesChandan MishraAinda não há avaliações
- Parkinson Drug TherapyDocumento20 páginasParkinson Drug Therapympl.raol50% (2)
- NCP PretermDocumento5 páginasNCP PretermJamine Joyce Ortega-AlvarezAinda não há avaliações
- NCP Disturbed Body ImageDocumento5 páginasNCP Disturbed Body ImageAira AlaroAinda não há avaliações
- High Alert MedicationsDocumento1 páginaHigh Alert MedicationsrsdsAinda não há avaliações
- Olsson Et Al (2010) Experiences in Close Relationships Measure of Adult AttachmentDocumento11 páginasOlsson Et Al (2010) Experiences in Close Relationships Measure of Adult AttachmentJR AlarcónAinda não há avaliações
- Cancer Industry, The Classic Expose of The - Moss, Ralph WDocumento546 páginasCancer Industry, The Classic Expose of The - Moss, Ralph Wpdf ebook free download80% (5)
- CB5c Cardiovascular Disease: Answer The Questions BelowDocumento24 páginasCB5c Cardiovascular Disease: Answer The Questions Belowseema chaturvediAinda não há avaliações
- Immunotec Whey To Go!: Immunotec Is Building An Empire On Patented ResultsDocumento5 páginasImmunotec Whey To Go!: Immunotec Is Building An Empire On Patented Resultsapi-26034055Ainda não há avaliações
- Nightingale Medical Trust Concessions For Senior CitizensDocumento40 páginasNightingale Medical Trust Concessions For Senior CitizensrnctechAinda não há avaliações
- Nursing Care For Patients With Ear, Eye, Nose &throat2Documento37 páginasNursing Care For Patients With Ear, Eye, Nose &throat2JSeashark100% (1)