Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Drug Elimination: Termination of Drug ActionDocumento80 páginasDrug Elimination: Termination of Drug ActionLidyaAinda não há avaliações
- Introduction To Cell BiologyDocumento32 páginasIntroduction To Cell BiologyMustafa Khandgawi100% (3)
- (20493614 - Endocrine Connections) How Glucagon-Like Peptide 1 Receptor Agonists WorkDocumento13 páginas(20493614 - Endocrine Connections) How Glucagon-Like Peptide 1 Receptor Agonists WorkEka RahmawatiAinda não há avaliações
- Anatomy Physiology and Disease For The Health Professions 3rd Edition Booth Wyman Stoia Test BankDocumento38 páginasAnatomy Physiology and Disease For The Health Professions 3rd Edition Booth Wyman Stoia Test Bankblair100% (25)
- SEMINAR HypoxiaDocumento28 páginasSEMINAR HypoxiaMalikAinda não há avaliações
- Test Bank For Molecular Biology Principles and Practice 1st Edition Michael M CoxDocumento6 páginasTest Bank For Molecular Biology Principles and Practice 1st Edition Michael M CoxglendavictoriabbkAinda não há avaliações
- Cornell Notes 4Documento3 páginasCornell Notes 4api-330067852Ainda não há avaliações
- Peptide HandbookDocumento26 páginasPeptide HandbookKim HiềnAinda não há avaliações
- Learning Activity 1 CarbohydratesDocumento59 páginasLearning Activity 1 CarbohydratesMaxine Danielle AlmeroAinda não há avaliações
- Carbohydrate Mcas Questions 1 2015Documento3 páginasCarbohydrate Mcas Questions 1 2015api-263230840Ainda não há avaliações
- What Is A GeneDocumento11 páginasWhat Is A GeneetdsdgAinda não há avaliações
- Pet 15 BMDocumento2 páginasPet 15 BMNick FisherAinda não há avaliações
- Chapter 10Documento45 páginasChapter 10api-44486912Ainda não há avaliações
- CHE631-Module 5 - Nucleic AcidDocumento22 páginasCHE631-Module 5 - Nucleic AcidrutwickAinda não há avaliações
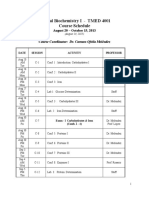
- Clinical Biochemistry I - TMED 4001 Course Schedule: Course Coordinator: Dr. Carmen Ofelia MeléndezDocumento3 páginasClinical Biochemistry I - TMED 4001 Course Schedule: Course Coordinator: Dr. Carmen Ofelia MeléndezNb + XB = AVAinda não há avaliações
- Lecture 2 Enzyme KineticsDocumento31 páginasLecture 2 Enzyme KineticsCarinaJongLeeAinda não há avaliações
- Interrelationship Between Carbohydrate Protein Fat MetabolismDocumento12 páginasInterrelationship Between Carbohydrate Protein Fat MetabolismShailaja Neaupane100% (5)
- Biomolecules 13 00441 v2Documento23 páginasBiomolecules 13 00441 v2Sarah SalaAinda não há avaliações
- Unit 1 Biology IAL Past Papers by TopicDocumento23 páginasUnit 1 Biology IAL Past Papers by TopicWillie Wong100% (2)
- Mader Chap012 10eTBDocumento17 páginasMader Chap012 10eTBDr. Michael DavidAinda não há avaliações
- Lecture 6 Overview of Cellular EnergyDocumento56 páginasLecture 6 Overview of Cellular EnergyMaimouna DialloAinda não há avaliações
- Chitosan Nanoparticles For Oral Drug and Gene DeliveryDocumento12 páginasChitosan Nanoparticles For Oral Drug and Gene DeliveryIoana-Cristina CarlanAinda não há avaliações
- Long Term Follow Up After Admin Human GT Products - Jan - 2020Documento37 páginasLong Term Follow Up After Admin Human GT Products - Jan - 2020DAinda não há avaliações
- Antimicrobial AgentsDocumento4 páginasAntimicrobial Agents13bellsAinda não há avaliações
- Electrophoresis: Food Analysis and Biochemistry-PracticeDocumento41 páginasElectrophoresis: Food Analysis and Biochemistry-PracticesusandhikaAinda não há avaliações
- Recent Trends in Chikungunya Virus DiagnosisDocumento8 páginasRecent Trends in Chikungunya Virus DiagnosisArpanaNiranjanAinda não há avaliações
- BIOC2014: Data From Testing The Yeast Invertase Experiment, Sept. 2020Documento6 páginasBIOC2014: Data From Testing The Yeast Invertase Experiment, Sept. 2020lakadia taylorAinda não há avaliações
- 2021-Rates of Contributory de Novo Mutation in High and Low-Risk Autism Families.Documento10 páginas2021-Rates of Contributory de Novo Mutation in High and Low-Risk Autism Families.熊佳仪(不冬眠的熊)Ainda não há avaliações
- CBSE Class 11 Biology Cell Cycle and Cell Division NotesDocumento4 páginasCBSE Class 11 Biology Cell Cycle and Cell Division NotesVansh MehtaAinda não há avaliações
- Golden RiceDocumento1 páginaGolden Ricedoris_1987Ainda não há avaliações