Você também pode gostar
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Neuroscience: Science of The BrainDocumento60 páginasNeuroscience: Science of The BrainInternational Brain Research Organization89% (76)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- A Critical Appreciation of Ode To NightingaleDocumento3 páginasA Critical Appreciation of Ode To NightingaleBaloch Karawan100% (2)
- The Emom Manual: 25 Kettlebell Conditioning WorkoutsDocumento14 páginasThe Emom Manual: 25 Kettlebell Conditioning WorkoutsguilleAinda não há avaliações
- Nta855 C400 D6 PDFDocumento110 páginasNta855 C400 D6 PDFIsmael Grünhäuser100% (4)
- Control of Corrosion in Cooling Waters PDFDocumento93 páginasControl of Corrosion in Cooling Waters PDFVictor SabAinda não há avaliações
- Refinería Kirkuk PDFDocumento11 páginasRefinería Kirkuk PDFcesarinarragaAinda não há avaliações
- Appendix B - Distance Tables - Metric Units PDFDocumento15 páginasAppendix B - Distance Tables - Metric Units PDFitisIAinda não há avaliações
- Given The Simulation Area For Room ServiceDocumento3 páginasGiven The Simulation Area For Room ServiceRico EsponillaAinda não há avaliações
- Catalysis For Co2 Conversion A Key Technology For Rapid Introduction of Renewable Energy in The Value Chain of Chemical IndustriesDocumento20 páginasCatalysis For Co2 Conversion A Key Technology For Rapid Introduction of Renewable Energy in The Value Chain of Chemical IndustriesVictor SabAinda não há avaliações
- EVO Series UserGuideDocumento59 páginasEVO Series UserGuideVictor SabAinda não há avaliações
- Basics of Electrochemical Impedance SpectrosDocumento36 páginasBasics of Electrochemical Impedance SpectrosSourabh AgrawalAinda não há avaliações
- Cuerpos Sin Edad, Mentes Sin Tiempo - Deepak ChopraDocumento108 páginasCuerpos Sin Edad, Mentes Sin Tiempo - Deepak ChopraVictor Sab0% (1)
- Evaluation of Microhardness and PDFDocumento7 páginasEvaluation of Microhardness and PDFVictor SabAinda não há avaliações
- Articulo 8 Water ResearchDocumento11 páginasArticulo 8 Water ResearchVictor SabAinda não há avaliações
- Evaluation of Microhardness andDocumento1 páginaEvaluation of Microhardness andVictor SabAinda não há avaliações
- Fluid Dynamics and Transport of PDFDocumento3 páginasFluid Dynamics and Transport of PDFVictor SabAinda não há avaliações
- A Study of Nickel Based CorrosioDocumento5 páginasA Study of Nickel Based CorrosioVictor SabAinda não há avaliações
- Fluid Dynamics and Transport ofDocumento5 páginasFluid Dynamics and Transport ofVictor SabAinda não há avaliações
- Characterization of Thermal SprayDocumento4 páginasCharacterization of Thermal SprayVictor SabAinda não há avaliações
- Sunlight Innovation ChallengeDocumento2 páginasSunlight Innovation ChallengeVictor SabAinda não há avaliações
- Electrochemical Impedance Models For Molten Salt Corrosion: C.L. Zeng, W. Wang, W.T. WuDocumento15 páginasElectrochemical Impedance Models For Molten Salt Corrosion: C.L. Zeng, W. Wang, W.T. WuVictor SabAinda não há avaliações
- Alternative Methodology For On Site Monitoring of Corrosion and Remediation of Reinforced ConcreteDocumento7 páginasAlternative Methodology For On Site Monitoring of Corrosion and Remediation of Reinforced ConcreteVictor SabAinda não há avaliações
- Junkyard Battery v2 Muralidharan2016Documento8 páginasJunkyard Battery v2 Muralidharan2016Eric S100% (1)
- Alternative Methodology For On Site Monitoring of Corrosion and Remediation of Reinforced ConcreteDocumento8 páginasAlternative Methodology For On Site Monitoring of Corrosion and Remediation of Reinforced ConcreteVictor SabAinda não há avaliações
- Characterization of Thermal Spray CoatingsDocumento8 páginasCharacterization of Thermal Spray Coatingsrkkumarcpri100% (1)
- Gamry The Basics of EIS Part 1Documento18 páginasGamry The Basics of EIS Part 1Mobasher KhanAinda não há avaliações
- Biomateriale Metalice Utilizate La Executia Tijelor Centromedulare ZavorateDocumento12 páginasBiomateriale Metalice Utilizate La Executia Tijelor Centromedulare ZavorateVictor SabAinda não há avaliações
- Alternative Methodology For On Site Monitoring of Corrosion and Remediation of Reinforced ConcreteDocumento7 páginasAlternative Methodology For On Site Monitoring of Corrosion and Remediation of Reinforced ConcreteVictor SabAinda não há avaliações
- Biofuels Innovation CallengeDocumento2 páginasBiofuels Innovation CallengeVictor SabAinda não há avaliações
- Characteristic Analysis of ZnO Varistors Made With Spherical Precipitation PowdersDocumento6 páginasCharacteristic Analysis of ZnO Varistors Made With Spherical Precipitation PowdersVictor SabAinda não há avaliações
- Automatic GunsDocumento1 páginaAutomatic GunsVictor SabAinda não há avaliações
- Biofuels Innovation CallengeDocumento2 páginasBiofuels Innovation CallengeVictor SabAinda não há avaliações
- Biohydrogen Production From Waste BiomassDocumento2 páginasBiohydrogen Production From Waste BiomassVictor SabAinda não há avaliações
- Characterization of Thermal Spray CoatingsDocumento8 páginasCharacterization of Thermal Spray CoatingsVictor SabAinda não há avaliações
- Comparative Characteristics of Yttrium Oxide and Ytrium Acid Nitric On Zno VaristorsDocumento7 páginasComparative Characteristics of Yttrium Oxide and Ytrium Acid Nitric On Zno VaristorsVictor SabAinda não há avaliações
- Electromagnetic Spectrum 1 QP PDFDocumento13 páginasElectromagnetic Spectrum 1 QP PDFWai HponeAinda não há avaliações
- Phardose Lab Prep 19 30Documento4 páginasPhardose Lab Prep 19 30POMPEYO BARROGAAinda não há avaliações
- Bai Tap Tieng Anh Lop 8 (Bai 13)Documento4 páginasBai Tap Tieng Anh Lop 8 (Bai 13)nguyenanhmaiAinda não há avaliações
- Plica PDFDocumento7 páginasPlica PDFIVAN VERGARAAinda não há avaliações
- Employment Offer: 1. Employer InformationDocumento2 páginasEmployment Offer: 1. Employer InformationnavidAinda não há avaliações
- Gendec - Inbound HS-HTNDocumento1 páginaGendec - Inbound HS-HTNKhalidAinda não há avaliações
- Registration Statement (For Single Proprietor)Documento2 páginasRegistration Statement (For Single Proprietor)Sherwin SalanayAinda não há avaliações
- Chemistry Xi: Short Questions and 20% Long QuestionsDocumento3 páginasChemistry Xi: Short Questions and 20% Long QuestionsSyed Nabeel HassanAinda não há avaliações
- Uas MR1Documento2 páginasUas MR1IvanAinda não há avaliações
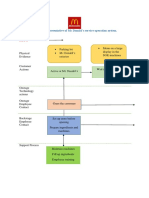
- Blueprint Huynh My Ky Duyen 2022 McDonald'sDocumento2 páginasBlueprint Huynh My Ky Duyen 2022 McDonald'sHuỳnh Mỹ Kỳ DuyênAinda não há avaliações
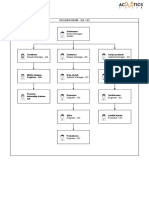
- Organogram - Qa / QC: Srinivasan SrinivasanDocumento4 páginasOrganogram - Qa / QC: Srinivasan SrinivasanGowtham VenkatAinda não há avaliações
- ZJZJP Roots Vauum PumpDocumento8 páginasZJZJP Roots Vauum PumpAnonymous Tj3ApePIrAinda não há avaliações
- Education in America: The Dumbing Down of The U.S. Education SystemDocumento4 páginasEducation in America: The Dumbing Down of The U.S. Education SystemmiichaanAinda não há avaliações
- Null 6 PDFDocumento1 páginaNull 6 PDFSimbarashe ChikariAinda não há avaliações
- Unit 8 Packet KeyDocumento21 páginasUnit 8 Packet KeyHiddenAinda não há avaliações
- TC 10 emDocumento7 páginasTC 10 emDina LydaAinda não há avaliações
- Oil ShaleDocumento13 páginasOil Shalergopi_83Ainda não há avaliações
- FINAL PAPER Marketing Plan For Rainbow Air PurifierDocumento12 páginasFINAL PAPER Marketing Plan For Rainbow Air PurifierMohola Tebello Griffith100% (1)
- Money Tree International Finance Corp. Checklist of Standard Loan RequirementsDocumento2 páginasMoney Tree International Finance Corp. Checklist of Standard Loan RequirementsAgape LabuntogAinda não há avaliações
- Eric Koech CV - Docx..bakDocumento7 páginasEric Koech CV - Docx..bakPeter Osundwa KitekiAinda não há avaliações
- CBEU Service ConditionsDocumento623 páginasCBEU Service ConditionsAtul ModiAinda não há avaliações
- Starkville Dispatch Eedition 9-10-20Documento12 páginasStarkville Dispatch Eedition 9-10-20The DispatchAinda não há avaliações
- G1 Series User Manual Ver. 1.2Documento101 páginasG1 Series User Manual Ver. 1.2unedo parhusip100% (1)
- 2020 ROTH IRA 229664667 Form 5498Documento2 páginas2020 ROTH IRA 229664667 Form 5498hk100% (1)