Você também pode gostar
- Pead 3 - Abdominal Pain and VommitingDocumento22 páginasPead 3 - Abdominal Pain and Vommitingbbyes100% (1)
- Guideline: Maternity - Maternal Group B Streptococcus (GBS) and Minimisation of Neonatal Early-Onset GBS SepsisDocumento18 páginasGuideline: Maternity - Maternal Group B Streptococcus (GBS) and Minimisation of Neonatal Early-Onset GBS SepsisbbyesAinda não há avaliações
- Pead 1 - NeonatologyDocumento21 páginasPead 1 - NeonatologybbyesAinda não há avaliações
- Early Pregnancy ComplciationsDocumento43 páginasEarly Pregnancy ComplciationsbbyesAinda não há avaliações
- Prenatal ScreeningDocumento26 páginasPrenatal ScreeningbbyesAinda não há avaliações
- Advanced Life Support AssessmentDocumento1 páginaAdvanced Life Support AssessmentbbyesAinda não há avaliações
- Tocolytics in PretermDocumento13 páginasTocolytics in PretermbbyesAinda não há avaliações
- Substance Abuse in PregnancyDocumento151 páginasSubstance Abuse in PregnancybbyesAinda não há avaliações
- HMO Surgical PositionDocumento4 páginasHMO Surgical PositionbbyesAinda não há avaliações
- SSIC Program of Delivery: Should Be Completed (Week) Date Orientation Evening and Entrance ExamDocumento4 páginasSSIC Program of Delivery: Should Be Completed (Week) Date Orientation Evening and Entrance ExambbyesAinda não há avaliações
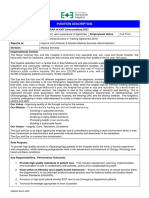
- Position Description ENTDocumento3 páginasPosition Description ENTbbyesAinda não há avaliações
- BASIC Course Gosford June 2021Documento3 páginasBASIC Course Gosford June 2021bbyesAinda não há avaliações
- Training Manual 2020Documento53 páginasTraining Manual 2020bbyesAinda não há avaliações
- Surgical - Information GuideDocumento2 páginasSurgical - Information GuidebbyesAinda não há avaliações
- Atrial Fibrillation Managing Acute Atrial FibrillationDocumento8 páginasAtrial Fibrillation Managing Acute Atrial FibrillationbbyesAinda não há avaliações
- Upper GI BleedDocumento8 páginasUpper GI BleedbbyesAinda não há avaliações
- C SpineDocumento44 páginasC SpinebbyesAinda não há avaliações
- Ischkwa DiagramDocumento1 páginaIschkwa DiagrambbyesAinda não há avaliações
- Organisation Chart - TraineeDocumento1 páginaOrganisation Chart - TraineebbyesAinda não há avaliações
- Right VATS Pleural BiopsyDocumento4 páginasRight VATS Pleural BiopsybbyesAinda não há avaliações
- Varicose VeinDocumento6 páginasVaricose VeinbbyesAinda não há avaliações
- RHDDocumento130 páginasRHDDeepu RajendranAinda não há avaliações
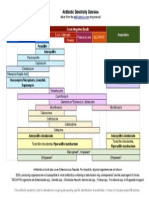
- Antibiotic Sensitivity Overview: Gram Positive Cocci Gram Negative Bacilli AnaerobesDocumento1 páginaAntibiotic Sensitivity Overview: Gram Positive Cocci Gram Negative Bacilli AnaerobesGuillermo Damian RodriguezAinda não há avaliações
- Infections in PregnancyDocumento11 páginasInfections in PregnancybbyesAinda não há avaliações
- Weekly SDS Topics: Week 3Documento1 páginaWeekly SDS Topics: Week 3bbyesAinda não há avaliações
- Shoulder PainDocumento5 páginasShoulder PainbbyesAinda não há avaliações
- Pump Manual TextDocumento17 páginasPump Manual TextbbyesAinda não há avaliações
- ECGs - UpdatedDocumento26 páginasECGs - UpdatedbbyesAinda não há avaliações
- Main Presentations of Sexually Transmitted Infections in MenDocumento3 páginasMain Presentations of Sexually Transmitted Infections in MenbbyesAinda não há avaliações
- Prof PracDocumento3 páginasProf PracbbyesAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- START Triage Training Presentation TTT 8 31 - 1 PDFDocumento95 páginasSTART Triage Training Presentation TTT 8 31 - 1 PDFCM NajitoAinda não há avaliações
- Structure in The Kite RunnerDocumento4 páginasStructure in The Kite Runnerushi12Ainda não há avaliações
- Biomechanics of Cycling: (Literature Review)Documento24 páginasBiomechanics of Cycling: (Literature Review)Marcelo CarvalhoAinda não há avaliações
- Tool Operating Manual Tool Operating Manual: 276-7273 Cylinder Sensor Test Box (In Cylinder Function Test)Documento12 páginasTool Operating Manual Tool Operating Manual: 276-7273 Cylinder Sensor Test Box (In Cylinder Function Test)CarlosAinda não há avaliações
- Contractor Health and Safety Manual: February 2019Documento21 páginasContractor Health and Safety Manual: February 2019Heru MulyonoAinda não há avaliações
- ZAMIL PY Series Installation, Operation & Maintenance ManualDocumento33 páginasZAMIL PY Series Installation, Operation & Maintenance Manualambuenaflor67% (9)
- Affidavit Complaint Slight Physical InjuryDocumento2 páginasAffidavit Complaint Slight Physical Injuryduanepo100% (1)
- Sketetal SystemDocumento11 páginasSketetal SystemBryan JagroopAinda não há avaliações
- Hip Disloc and Fem HeadDocumento60 páginasHip Disloc and Fem HeadZisuhAinda não há avaliações
- 500 Spanish VerbsDocumento25 páginas500 Spanish VerbshashemAinda não há avaliações
- Pedal Cycle Helmet Position Paper FinalDocumento2 páginasPedal Cycle Helmet Position Paper FinaljusendqAinda não há avaliações
- Briggs and Stratton 500EDocumento116 páginasBriggs and Stratton 500EFunnypoumAinda não há avaliações
- Operator Manual: Generator SetDocumento74 páginasOperator Manual: Generator SetManoelAinda não há avaliações
- ARDSDocumento81 páginasARDSShanaz NovriandinaAinda não há avaliações
- Neuroimaging of Spinal Instability-Journal ReadingDocumento18 páginasNeuroimaging of Spinal Instability-Journal ReadingAmanda Aldilla MeutiadiAinda não há avaliações
- Jigy WirgleDocumento486 páginasJigy Wirglesierleinad1Ainda não há avaliações
- Working at Shuttering Yard JSA HSE ProfessionalsDocumento2 páginasWorking at Shuttering Yard JSA HSE ProfessionalsViron BaxhiaAinda não há avaliações
- Zafehouse Diaries - ManualDocumento45 páginasZafehouse Diaries - ManualHelder LinharesAinda não há avaliações
- Bone MuscleDocumento433 páginasBone Muscleridho budiAinda não há avaliações
- RIB FractureDocumento46 páginasRIB Fracturebanjar1982Ainda não há avaliações
- CAHB-20 Operating Manual enDocumento60 páginasCAHB-20 Operating Manual enDavid Lay IIAinda não há avaliações
- Brachial Plexus InjuryDocumento10 páginasBrachial Plexus InjurySanditya FadliAinda não há avaliações
- Contusio PulmonumDocumento10 páginasContusio PulmonumSyamsuriWahyuAinda não há avaliações
- From EFT To The Palace of Possibilities - Workshop Manual PDFDocumento61 páginasFrom EFT To The Palace of Possibilities - Workshop Manual PDFronaldolaux100% (2)
- CBD Clinic Massage Oil 12oz 11.7.18Documento1 páginaCBD Clinic Massage Oil 12oz 11.7.18Jose MaldonadoAinda não há avaliações
- DR - Sundeep Jeten RajDocumento32 páginasDR - Sundeep Jeten Rajselva3333Ainda não há avaliações
- Air & Space Law AssignmentDocumento5 páginasAir & Space Law AssignmentPartha Mehrotra100% (1)
- KWA-300 3D Wheel Aligner User's Manual enDocumento34 páginasKWA-300 3D Wheel Aligner User's Manual enJorge Eduardo Diaz ValenzuelaAinda não há avaliações
- ComplaintDocumento5 páginasComplaintShericka Jade MontorAinda não há avaliações
- ABC Guide To Temporary Pipework-Feb 2012 Rev5-SDocumento84 páginasABC Guide To Temporary Pipework-Feb 2012 Rev5-SKwesi Edwards100% (2)