Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Prognostication and Goals of Care Decisions in Severe Traumatic Brain InjuryDocumento52 páginasPrognostication and Goals of Care Decisions in Severe Traumatic Brain InjurygiseladlrAinda não há avaliações
- 2023 - Guidelines For Neuroprognostication in Adults With Guillain-Barré SyndromeDocumento20 páginas2023 - Guidelines For Neuroprognostication in Adults With Guillain-Barré SyndromegiseladlrAinda não há avaliações
- 2021 - Editor - Evidence Based Care For Individuals With Spinal Cord Injury Role of The Clinical Practice GuidelinesDocumento3 páginas2021 - Editor - Evidence Based Care For Individuals With Spinal Cord Injury Role of The Clinical Practice GuidelinesgiseladlrAinda não há avaliações
- 2023 - Hydrocortisone in Severe CommunityDocumento11 páginas2023 - Hydrocortisone in Severe CommunitygiseladlrAinda não há avaliações
- The Patient Needing Prolonged Mechanical VentilationDocumento10 páginasThe Patient Needing Prolonged Mechanical VentilationgiseladlrAinda não há avaliações
- 2023 - Optimal Oxygen and Mean Arterial Blood Pressure TargetsDocumento3 páginas2023 - Optimal Oxygen and Mean Arterial Blood Pressure TargetsgiseladlrAinda não há avaliações
- 2023 - Blood Pressure Management in IschemicDocumento10 páginas2023 - Blood Pressure Management in IschemicgiseladlrAinda não há avaliações
- 2023 - Hydrocortisone in Severe CommunityDocumento11 páginas2023 - Hydrocortisone in Severe CommunitygiseladlrAinda não há avaliações
- 2023 - It Takes An Average of 17 Years For Evidence To Change PracticeDocumento4 páginas2023 - It Takes An Average of 17 Years For Evidence To Change PracticegiseladlrAinda não há avaliações
- 2023 - Consequences of Spinal Cord Injury On The Sympathetic Nervous SystemDocumento26 páginas2023 - Consequences of Spinal Cord Injury On The Sympathetic Nervous SystemgiseladlrAinda não há avaliações
- 2022 - Fluid Management in Dengue Critical PhaseDocumento7 páginas2022 - Fluid Management in Dengue Critical PhasegiseladlrAinda não há avaliações
- Nejmra 2207410Documento15 páginasNejmra 2207410rindayusticia100% (1)
- 2022_Factors Associated With Spontaneous Awakening Trial and Spontaneous Breathing Trial Performance in Adults With Critical Illness_ Analysis of a Multicenter, Nationwide, Cohort Study - ScienceDirectDocumento5 páginas2022_Factors Associated With Spontaneous Awakening Trial and Spontaneous Breathing Trial Performance in Adults With Critical Illness_ Analysis of a Multicenter, Nationwide, Cohort Study - ScienceDirectgiseladlrAinda não há avaliações
- Escalaje de Vasopresores y Esteroides en Choque SépticoDocumento9 páginasEscalaje de Vasopresores y Esteroides en Choque SépticoTiziano DiCarloAinda não há avaliações
- 2023 - Pharmacokinetic Alterations Associated With Critical IllnessDocumento12 páginas2023 - Pharmacokinetic Alterations Associated With Critical IllnessgiseladlrAinda não há avaliações
- 2014 - Effectiveness of Implementing A Wake Up and Breathe ProgramDocumento10 páginas2014 - Effectiveness of Implementing A Wake Up and Breathe ProgramgiseladlrAinda não há avaliações
- 2023 - Lower Versus Higher Exposure To Vasopressor Therapy in Vasodilatory Hypotension RSL With Meta-AnalysisDocumento13 páginas2023 - Lower Versus Higher Exposure To Vasopressor Therapy in Vasodilatory Hypotension RSL With Meta-AnalysisgiseladlrAinda não há avaliações
- 2014 - The Preventability of Ventilator-Associated EventsDocumento10 páginas2014 - The Preventability of Ventilator-Associated EventsgiseladlrAinda não há avaliações
- 2023 - Epidemiology and Outcomes of Hospital Acquired Bloodstream Infections in Intensive Care Unit Patients The EUROBACT 2Documento13 páginas2023 - Epidemiology and Outcomes of Hospital Acquired Bloodstream Infections in Intensive Care Unit Patients The EUROBACT 2giseladlrAinda não há avaliações
- 2023 - Advanced Point-Of-Care Bedside Monitoring For Acute Respiratory FailureDocumento18 páginas2023 - Advanced Point-Of-Care Bedside Monitoring For Acute Respiratory FailuregiseladlrAinda não há avaliações
- D-Dimer Is A Significant Prognostic Factor in Patients With Suspected Infection and SepsisDocumento9 páginasD-Dimer Is A Significant Prognostic Factor in Patients With Suspected Infection and SepsisgiseladlrAinda não há avaliações
- 2022 - American Society of Transplant Surgeons Recommendations On Best Practices in Donation After Circulatory Death Organ ProcurementDocumento9 páginas2022 - American Society of Transplant Surgeons Recommendations On Best Practices in Donation After Circulatory Death Organ ProcurementgiseladlrAinda não há avaliações
- 2020 Global epidemiology of coronavirus disease 2019 (COVID-19)_ disease incidence, daily cumulative index, mortality, and their association with country healthcare resources and economic status - 1-s2.0-S0924857920300960-mainDocumento8 páginas2020 Global epidemiology of coronavirus disease 2019 (COVID-19)_ disease incidence, daily cumulative index, mortality, and their association with country healthcare resources and economic status - 1-s2.0-S0924857920300960-maingiseladlrAinda não há avaliações
- Efficacy of Electrical Muscle StimulatioDocumento212 páginasEfficacy of Electrical Muscle StimulatiogiseladlrAinda não há avaliações
- Proning in ARDSDocumento10 páginasProning in ARDSAndrew DavidsonAinda não há avaliações
- COVID-19 in The Eastern Mediterranean Region and Saudi Arabia - Prevention and Therapeutic Strategies - 1-S2.0-S0924857920301254-MainDocumento8 páginasCOVID-19 in The Eastern Mediterranean Region and Saudi Arabia - Prevention and Therapeutic Strategies - 1-S2.0-S0924857920301254-MaingiseladlrAinda não há avaliações
- Association Between Site of Infection and In-Hospital Mortality in Patients With Sepsis Admitted To Emergency Departments of Tertiary Hospitals in Medellin, ColombiaDocumento10 páginasAssociation Between Site of Infection and In-Hospital Mortality in Patients With Sepsis Admitted To Emergency Departments of Tertiary Hospitals in Medellin, ColombiagiseladlrAinda não há avaliações
- An Approach To Hemodynamic Monitoring SubrayadaDocumento7 páginasAn Approach To Hemodynamic Monitoring SubrayadagiseladlrAinda não há avaliações
- 2020 A Review of The 2019 Novel Coronavirus (COVID-19) Based On Current Evidence - 1-S2.0-S0924857920300984-MainDocumento31 páginas2020 A Review of The 2019 Novel Coronavirus (COVID-19) Based On Current Evidence - 1-S2.0-S0924857920300984-MaingiseladlrAinda não há avaliações
- BARICITINIB - A JANUASE KINASE INHIBITOR - NOT AN IDEAL OPTION FOR MANAGEMENT OF COVID 19 - 1-S2.0-S0924857920301242-MainDocumento9 páginasBARICITINIB - A JANUASE KINASE INHIBITOR - NOT AN IDEAL OPTION FOR MANAGEMENT OF COVID 19 - 1-S2.0-S0924857920301242-MaingiseladlrAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
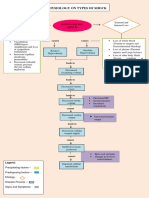
- Pathophysiology On Types of ShockDocumento4 páginasPathophysiology On Types of ShockJessa Mae Alforque AsentistaAinda não há avaliações
- Critical Care Nursing Diagnosis and Management 8th EditionDocumento61 páginasCritical Care Nursing Diagnosis and Management 8th Editionsharon.correia689100% (41)
- Merrill's Atlas of Radiographic Positions, Volume 2, 10th EditionDocumento514 páginasMerrill's Atlas of Radiographic Positions, Volume 2, 10th Editionchanyeol100% (2)
- Vol3 No 7 ATLS PDFDocumento10 páginasVol3 No 7 ATLS PDFlinaAinda não há avaliações
- Engebretsen2011, INSULINA EN B BLOQDocumento7 páginasEngebretsen2011, INSULINA EN B BLOQFabiola Delia Rosas AlarcónAinda não há avaliações
- Post Op CareDocumento21 páginasPost Op Careahmadkhanmansoor09Ainda não há avaliações
- Nurse EcmoDocumento124 páginasNurse EcmoSalvatore Cimino100% (5)
- Septic ShockDocumento11 páginasSeptic ShockJonna Mae Agcaoili SalameroAinda não há avaliações
- Hemo Dynamic Disorders Thrombo Embolism and ShockDocumento29 páginasHemo Dynamic Disorders Thrombo Embolism and ShockMai ÜüAinda não há avaliações
- Vasoconstriction in Septic Shock: What'S New in Intensive CareDocumento4 páginasVasoconstriction in Septic Shock: What'S New in Intensive CareGabriela PachecoAinda não há avaliações
- Sepsis and Septic ShockDocumento14 páginasSepsis and Septic Shocknursaidah100% (1)
- Obstructive Shock, From Diagnosis To TreatmentDocumento10 páginasObstructive Shock, From Diagnosis To TreatmentJonathan PuenteAinda não há avaliações
- Cardiovascular Pharmacology PDFDocumento20 páginasCardiovascular Pharmacology PDFMelanie PrinceAinda não há avaliações
- General Surgery MCQsDocumento16 páginasGeneral Surgery MCQssk91% (11)
- CME UGIB, Hypovolemic Shock 31.12.21 - FINALDocumento58 páginasCME UGIB, Hypovolemic Shock 31.12.21 - FINALThayalan RaviAinda não há avaliações
- Fluid Therapy and ShockDocumento8 páginasFluid Therapy and ShockJuan Francisco SánchezAinda não há avaliações
- Case 13 - People v. Ulep, G.R. No. L-36858Documento5 páginasCase 13 - People v. Ulep, G.R. No. L-36858Jo-Al GealonAinda não há avaliações
- Abdominal Compartment Syndrome and Intra Abdominal.21 PDFDocumento9 páginasAbdominal Compartment Syndrome and Intra Abdominal.21 PDFFIA SlotAinda não há avaliações
- MCQs Surgery Liaqat-FarhanDocumento22 páginasMCQs Surgery Liaqat-Farhanasim shehzad100% (1)
- First Aid-PowerpointDocumento57 páginasFirst Aid-PowerpointMaria Crisbeth SanchezAinda não há avaliações
- Trends in Nmangement and Outcomes of Patients With Acute Myocardil Infarction Complicated by Cardiogenic ShockDocumento7 páginasTrends in Nmangement and Outcomes of Patients With Acute Myocardil Infarction Complicated by Cardiogenic ShockVICTOR EUCLIDES BRIONES MORALESAinda não há avaliações
- Latest Thesis Topics in OrthodonticsDocumento6 páginasLatest Thesis Topics in Orthodonticsnadugnlkd100% (2)
- Guía Manejo Del Shock 2023Documento67 páginasGuía Manejo Del Shock 2023Alvaro ArriagadaAinda não há avaliações
- ExodoniaDocumento184 páginasExodoniaMohsin HabibAinda não há avaliações
- NCLEX Boot Camp Plan to Pass in 75 QuestionsDocumento24 páginasNCLEX Boot Camp Plan to Pass in 75 QuestionsMariekris Sangalang100% (8)
- Arnica The Miracle Remedy - Case Records - HomeopathyandmoreDocumento23 páginasArnica The Miracle Remedy - Case Records - HomeopathyandmoreAshna100% (1)
- Kuliah Syok 2020 (DR Ahmad Yafiz Hasby SpAn)Documento48 páginasKuliah Syok 2020 (DR Ahmad Yafiz Hasby SpAn)RezaAinda não há avaliações
- FCCS - Pediatric Vs Adult ConsiderationDocumento13 páginasFCCS - Pediatric Vs Adult ConsiderationludiAinda não há avaliações
- Nelson Pediatrics Review (MCQS) 17edDocumento631 páginasNelson Pediatrics Review (MCQS) 17edGabrielle Maycock75% (8)
- Homoeopathic remedies for shock and traumaDocumento2 páginasHomoeopathic remedies for shock and traumaSuhas IngaleAinda não há avaliações