Você também pode gostar
- Random Memory Notebook Pages Page 119Documento1 páginaRandom Memory Notebook Pages Page 119angie10231Ainda não há avaliações
- Intramuscular Injection GuidelinesDocumento2 páginasIntramuscular Injection Guidelinesangie10231Ainda não há avaliações
- Random Memory Notebook Pages Page 121Documento1 páginaRandom Memory Notebook Pages Page 121angie10231Ainda não há avaliações
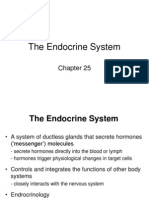
- 25 EndoDocumento66 páginas25 Endoangie10231Ainda não há avaliações
- Random Memory Notebook Pages Page 123Documento1 páginaRandom Memory Notebook Pages Page 123angie10231Ainda não há avaliações
- Endocrine System: Dr. Annette M. Parrott GPC BIOL1612Documento34 páginasEndocrine System: Dr. Annette M. Parrott GPC BIOL1612Nathan TaylorAinda não há avaliações
- Endocrine System: Hormones & HomeostasisDocumento32 páginasEndocrine System: Hormones & Homeostasisangie10231Ainda não há avaliações
- Random Memory Notebook Pages Page 124Documento1 páginaRandom Memory Notebook Pages Page 124angie10231Ainda não há avaliações
- Marieb ch7dDocumento17 páginasMarieb ch7dangie10231Ainda não há avaliações
- Random Memory Notebook Pages Page 128Documento1 páginaRandom Memory Notebook Pages Page 128angie10231Ainda não há avaliações
- Chapt17 StudentDocumento30 páginasChapt17 Studentangie10231Ainda não há avaliações
- Critical Thinking Flow Sheet For Nursing StudentsDocumento3 páginasCritical Thinking Flow Sheet For Nursing Studentsangie10231Ainda não há avaliações
- The Roles of Calcitonin, Parathyroid Hormone & CalcitrolDocumento7 páginasThe Roles of Calcitonin, Parathyroid Hormone & Calcitrolangie10231Ainda não há avaliações
- Endocrine SystemDocumento28 páginasEndocrine Systemangie10231Ainda não há avaliações
- Signal Transmission at A Chemical SynapseDocumento7 páginasSignal Transmission at A Chemical Synapseangie10231Ainda não há avaliações
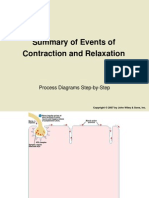
- Contraction & RelaxationDocumento10 páginasContraction & Relaxationangie10231Ainda não há avaliações
- General Components of A Reflex ArcDocumento6 páginasGeneral Components of A Reflex Arcangie10231Ainda não há avaliações
- Steps in Repair of A Bone Fracture: Process Diagrams Step-by-StepDocumento5 páginasSteps in Repair of A Bone Fracture: Process Diagrams Step-by-Steprambabs369Ainda não há avaliações
- Receptor-Mediated Endocytosis: Process Diagrams Step-by-StepDocumento7 páginasReceptor-Mediated Endocytosis: Process Diagrams Step-by-Steprambabs369Ainda não há avaliações
- Intramembranous Ossification: Process Diagrams Step-by-StepDocumento5 páginasIntramembranous Ossification: Process Diagrams Step-by-Steprambabs369Ainda não há avaliações
- Anatomy Study BinderDocumento13 páginasAnatomy Study Binderangie10231Ainda não há avaliações
- Olfactory Bulb Olfactory Tract Optic Nerve Optic Chiasma Optic Tract Pituitary Gland (Hypophysis) Frontal LobeDocumento1 páginaOlfactory Bulb Olfactory Tract Optic Nerve Optic Chiasma Optic Tract Pituitary Gland (Hypophysis) Frontal Lobeangie10231Ainda não há avaliações
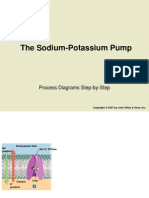
- The Sodium-Potassium Pump: Process Diagrams Step-by-StepDocumento5 páginasThe Sodium-Potassium Pump: Process Diagrams Step-by-Steprambabs369Ainda não há avaliações
- Structure of The Neuromuscular JunctionDocumento5 páginasStructure of The Neuromuscular Junctionangie10231Ainda não há avaliações
- LabValues (1) Nclex Review2Documento1 páginaLabValues (1) Nclex Review2angie10231Ainda não há avaliações
- Study Recommendations For HESI Admissions Assessment TestDocumento20 páginasStudy Recommendations For HESI Admissions Assessment TestNibin Varghese0% (1)
- Rbel60708 1-266241Documento28 páginasRbel60708 1-266241angie10231Ainda não há avaliações
- Dosage Calculation TutorialDocumento68 páginasDosage Calculation TutorialRon AbuAinda não há avaliações
- Hypophysis (Pituitary Gland)Documento1 páginaHypophysis (Pituitary Gland)angie10231Ainda não há avaliações
- Hesi Study GuideDocumento16 páginasHesi Study Guideangie10231100% (3)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (120)