Você também pode gostar
- CLINICAL HISTORY AND DIFFERENTIAL DIAGNOSIS AT YOUR FINGERTIPSNo EverandCLINICAL HISTORY AND DIFFERENTIAL DIAGNOSIS AT YOUR FINGERTIPSAinda não há avaliações
- Sem 3 Medical Science b4 ExmDocumento2 páginasSem 3 Medical Science b4 ExmKelly YeowAinda não há avaliações
- 3-Pharynx. OesophagusDocumento30 páginas3-Pharynx. OesophagusislamAinda não há avaliações
- 18 - Oncologic - Emergencies (PICU COURSE)Documento44 páginas18 - Oncologic - Emergencies (PICU COURSE)surasuarezlopezAinda não há avaliações
- Throat PowerpointDocumento29 páginasThroat Powerpointminci sensei100% (8)
- Surgery EORDocumento76 páginasSurgery EORAndrew BowmanAinda não há avaliações
- A UGI (Blue Keyword Pyq)Documento3 páginasA UGI (Blue Keyword Pyq)Irsyad SiddeeqAinda não há avaliações
- Test 2 NotesDocumento38 páginasTest 2 Notesbjpalmer100% (2)
- Surgical Disease of The Esophagus: Mahteme Bekele, MD Assistant Professor of SurgeryDocumento72 páginasSurgical Disease of The Esophagus: Mahteme Bekele, MD Assistant Professor of SurgeryBiniamAinda não há avaliações
- Cardiac Imaging TechniquesDocumento86 páginasCardiac Imaging Techniquesj.doe.hex_87Ainda não há avaliações
- Oesophagus StomachDocumento28 páginasOesophagus Stomachwanja91Ainda não há avaliações
- BOLILE ESOFAGUL Mia TareDocumento12 páginasBOLILE ESOFAGUL Mia Tareelisabeth-ward-skipAinda não há avaliações
- Tulburari FunctionaleDocumento158 páginasTulburari Functionalelleticia87Ainda não há avaliações
- Esophageal and Stomach Pathology-May+2019Documento71 páginasEsophageal and Stomach Pathology-May+2019Karami Brutus0% (1)
- DYSPHAGIA Lecture NotesDocumento84 páginasDYSPHAGIA Lecture Notesmcmak357Ainda não há avaliações
- Short Written Mock 2021 Mn1 - AnsweredDocumento20 páginasShort Written Mock 2021 Mn1 - AnsweredMatthew NgAinda não há avaliações
- DYSPHAGIA FINALgDocumento48 páginasDYSPHAGIA FINALgSurbhi BhartiAinda não há avaliações
- Gastroenterology by Elagouri MohammedDocumento31 páginasGastroenterology by Elagouri MohammedStylesh GuRlyAinda não há avaliações
- Basic Abdominal Ultrasound - BestDocumento36 páginasBasic Abdominal Ultrasound - Bestifeanyi100% (2)
- Ploughing Through PACES Collected by DR Azmy PDFDocumento385 páginasPloughing Through PACES Collected by DR Azmy PDFtejbirsingh2013Ainda não há avaliações
- ESOPHAGEAL:Gastritis DiseaseDocumento25 páginasESOPHAGEAL:Gastritis DiseaseraAinda não há avaliações
- Bachtiar Murtala: Department of Radiology Medical Faculty Hasanuddin UniversityDocumento102 páginasBachtiar Murtala: Department of Radiology Medical Faculty Hasanuddin UniversitynafisahAinda não há avaliações
- TBL 3: Dysphagia: By: Anis, Aishah, Nubla, Hanafi, HidayahDocumento84 páginasTBL 3: Dysphagia: By: Anis, Aishah, Nubla, Hanafi, HidayahNadia RahimAinda não há avaliações
- Bolile EsofagulDocumento13 páginasBolile Esofagulelisabeth-ward-skipAinda não há avaliações
- One Day Term Baby Born To Primi Brought With H/o Unable To Feed/ 'Chocking' and Excess Salivation From Mouth Diagnosis?Documento62 páginasOne Day Term Baby Born To Primi Brought With H/o Unable To Feed/ 'Chocking' and Excess Salivation From Mouth Diagnosis?lumina.sAinda não há avaliações
- Dysphagia and Oesophageal Carcinoma-Maj (DR) Francis KamunduDocumento44 páginasDysphagia and Oesophageal Carcinoma-Maj (DR) Francis KamunduKutemwaAinda não há avaliações
- The Liver: Methods of ExaminationDocumento49 páginasThe Liver: Methods of Examinationj.doe.hex_87Ainda não há avaliações
- Carcinoma of EsophagusDocumento13 páginasCarcinoma of EsophagusShujina ZainabAinda não há avaliações
- Barrett's, PVSDocumento16 páginasBarrett's, PVSNurulasyikin MAAAinda não há avaliações
- DysphagiaDocumento35 páginasDysphagiaBashar KhalilAinda não há avaliações
- Gastrointestinal PathologyDocumento14 páginasGastrointestinal PathologyRahul ShuklaAinda não há avaliações
- GI Sympt Mokhtar (2015)Documento85 páginasGI Sympt Mokhtar (2015)Abdelrahman MokhtarAinda não há avaliações
- Mock OSCE AnswersDocumento7 páginasMock OSCE AnswersUsama SabeehAinda não há avaliações
- Powerpoint: Disorders of The Esophagus IIDocumento43 páginasPowerpoint: Disorders of The Esophagus IIj.doe.hex_8767% (3)
- Common Complaints of Diseases of The AbdomenDocumento37 páginasCommon Complaints of Diseases of The AbdomenNorjetalexis Maningo CabreraAinda não há avaliações
- Esophagous Stomach Small Intestine PathologyDocumento58 páginasEsophagous Stomach Small Intestine PathologytahaAinda não há avaliações
- Dysphagia: DR S Jaya SandeepDocumento22 páginasDysphagia: DR S Jaya Sandeepsai kousikAinda não há avaliações
- Gastrointestinal System: Symptomatology of TheDocumento85 páginasGastrointestinal System: Symptomatology of TheAbdelrahman MokhtarAinda não há avaliações
- It 2 - Signs and Symptoms of Git DisordersDocumento54 páginasIt 2 - Signs and Symptoms of Git Disorderspikaanisa100% (9)
- Dyspepsia Lecture 6Documento28 páginasDyspepsia Lecture 6Dhante MRDAinda não há avaliações
- Thyroid Gland: Sheena Mae SangutanDocumento27 páginasThyroid Gland: Sheena Mae SangutanMarrah Avila Acuin100% (1)
- Look:: Gastrointestinal ExamDocumento6 páginasLook:: Gastrointestinal ExamTom MallinsonAinda não há avaliações
- GIT - EsophagusDocumento5 páginasGIT - EsophagussebarikattaAinda não há avaliações
- Aspek Medis Bedah (Perioperatif) Dan Enteral - Parenteral NutrisiDocumento56 páginasAspek Medis Bedah (Perioperatif) Dan Enteral - Parenteral NutrisiJashmine RachlyAinda não há avaliações
- Dysphagia: DR (Prof.) A B Singh Unit Department of General Surgery Patna Medical College & HospitalDocumento48 páginasDysphagia: DR (Prof.) A B Singh Unit Department of General Surgery Patna Medical College & HospitalAswin Rajasekaran100% (1)
- Radiology of Gastrointestinal Tract: (GIT) Bachtiar MurtalaDocumento53 páginasRadiology of Gastrointestinal Tract: (GIT) Bachtiar MurtalaMichael HusainAinda não há avaliações
- Alcoholism and HepatitisDocumento15 páginasAlcoholism and HepatitisTom MallinsonAinda não há avaliações
- GastroIntrology KuliahDocumento111 páginasGastroIntrology KuliahRenny WidiastutiAinda não há avaliações
- Hiatal HerniaDocumento63 páginasHiatal HerniaCandace LongAinda não há avaliações
- Peptic Ulcer DiseaseDocumento18 páginasPeptic Ulcer Diseasekhadzx100% (4)
- Fundamentals of NursingDocumento8 páginasFundamentals of NursingFreeNursingNotes92% (13)
- MED Diseases of The EsophagusDocumento4 páginasMED Diseases of The EsophagusJulie Anne AciertoAinda não há avaliações
- Parasitic Diseases in SurgeryDocumento60 páginasParasitic Diseases in SurgerySuvarna RajAinda não há avaliações
- Dysphagia and Carcinoma of The OesophagusDocumento14 páginasDysphagia and Carcinoma of The OesophagusCharles FrankAinda não há avaliações
- Ploughing Through PACESDocumento252 páginasPloughing Through PACESSmallsAinda não há avaliações
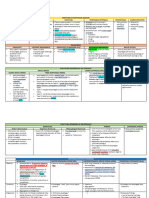
- DDX Gastrointestinal Disorders ChartDocumento20 páginasDDX Gastrointestinal Disorders ChartDavid UribeAinda não há avaliações
- Esophageal ConditionsDocumento43 páginasEsophageal ConditionsMICHAEL SAKALAAinda não há avaliações
- Acute Abdomen: Medic Curses A MopDocumento50 páginasAcute Abdomen: Medic Curses A MopSharaz AhmedAinda não há avaliações
- Gastro Intestinal Disorders:: Kawasaki DiseaseDocumento6 páginasGastro Intestinal Disorders:: Kawasaki DiseaseJoanna TaylanAinda não há avaliações
- Peptic Ulcer DiseaseDocumento18 páginasPeptic Ulcer DiseasechetankumarbhumireddyAinda não há avaliações
- Thomas SplintDocumento14 páginasThomas SplintNadia SalwaniAinda não há avaliações
- Spine ExaminationDocumento30 páginasSpine ExaminationNadia SalwaniAinda não há avaliações
- Referral Letter (19) HDFHFHDocumento2 páginasReferral Letter (19) HDFHFHNadia SalwaniAinda não há avaliações
- Immunization: Presenter: Ahmad Tahir Siti Nurul Farahah Supervised By: DR MuhaireenDocumento40 páginasImmunization: Presenter: Ahmad Tahir Siti Nurul Farahah Supervised By: DR MuhaireenNadia SalwaniAinda não há avaliações
- Paediatricshouseofficerguidehospitalkulim 151026150042 Lva1 App6891Documento14 páginasPaediatricshouseofficerguidehospitalkulim 151026150042 Lva1 App6891Nadia SalwaniAinda não há avaliações
- Sing To The Dawn, ChallengesDocumento1 páginaSing To The Dawn, ChallengesNadia Salwani100% (1)
- Respiratory Distress in NewbornDocumento52 páginasRespiratory Distress in NewbornNadia SalwaniAinda não há avaliações
- CKD History TakingDocumento2 páginasCKD History TakingNadia Salwani80% (5)
- Homework 16Documento1 páginaHomework 16Nadia SalwaniAinda não há avaliações
- Prostate CancerDocumento4 páginasProstate CancerNadia SalwaniAinda não há avaliações
- Blood Filtration and Nutrient and Water ReabsorptionDocumento2 páginasBlood Filtration and Nutrient and Water ReabsorptionNadia SalwaniAinda não há avaliações
- Soalan SeniorDocumento8 páginasSoalan SeniorNadia SalwaniAinda não há avaliações
- RadiologyDocumento1 páginaRadiologyNadia SalwaniAinda não há avaliações
- Headache: Red FlagsDocumento1 páginaHeadache: Red FlagsNadia SalwaniAinda não há avaliações
- Index NewwwwwwDocumento6 páginasIndex NewwwwwwNadia SalwaniAinda não há avaliações
- Headache, SkinDocumento4 páginasHeadache, SkinNadia SalwaniAinda não há avaliações
- Delicious Affordable Recharge Your EnergyDocumento1 páginaDelicious Affordable Recharge Your EnergyNadia SalwaniAinda não há avaliações
- Compusoft, 2 (3), 65-72Documento8 páginasCompusoft, 2 (3), 65-72Ravi Tyagi TyagiAinda não há avaliações
- The Facts On Sleep Apnea SecretsDocumento63 páginasThe Facts On Sleep Apnea SecretsClariceikoAinda não há avaliações
- Brain Computer InterfaceDocumento23 páginasBrain Computer InterfaceAmal TomAinda não há avaliações
- Anterolateral ThoracotomyDocumento6 páginasAnterolateral Thoracotomyfluid_man_brazilAinda não há avaliações
- MRCP EthicsDocumento33 páginasMRCP EthicstaherAinda não há avaliações
- Psychiatric Nursing SlidesDocumento27 páginasPsychiatric Nursing SlidesHazel RoseAinda não há avaliações
- Approach To Patient With FeverDocumento2 páginasApproach To Patient With FeverNonoy JoyaAinda não há avaliações
- UWorld Step3 CCS-1Documento13 páginasUWorld Step3 CCS-1Sarah LCAinda não há avaliações
- Ethical Issues in The Care of Older PersonsDocumento3 páginasEthical Issues in The Care of Older PersonsGodwin Babista GonzalesAinda não há avaliações
- Approach To Spontaneous PneumothoraxDocumento25 páginasApproach To Spontaneous PneumothoraxMohdGhazaliAcoyAinda não há avaliações
- dlt1107 1447a 1449Documento3 páginasdlt1107 1447a 1449abdulariifAinda não há avaliações
- CAP CURB-65 GuidelinesDocumento1 páginaCAP CURB-65 GuidelinesAndy LoakAinda não há avaliações
- SafePatientHandling PDFDocumento1 páginaSafePatientHandling PDFdipraAinda não há avaliações
- Management of Patients With Structural Infections and Inflammatory Cardiac Disorders Hinkle PPT CH 28Documento50 páginasManagement of Patients With Structural Infections and Inflammatory Cardiac Disorders Hinkle PPT CH 28DelindaEvans100% (4)
- Healthy Person ReportDocumento21 páginasHealthy Person ReportSwami AbhayanandAinda não há avaliações
- AMIDocumento44 páginasAMIsjamilmdfauzieAinda não há avaliações
- UW ObjectivesDocumento220 páginasUW ObjectivesRaymond Bernatowicz100% (2)
- Hypovolemia PresentationDocumento5 páginasHypovolemia PresentationjavibruinAinda não há avaliações
- Dialysis in Older PatientsDocumento220 páginasDialysis in Older PatientsMiguel Angel Molinero100% (1)
- Smiths Fluid Warmer - General Technical ManualDocumento131 páginasSmiths Fluid Warmer - General Technical Manualmeet_vaghaniAinda não há avaliações
- Objectives of Staffing in NursingDocumento10 páginasObjectives of Staffing in NursingEli Zza KoiralaAinda não há avaliações
- Acute Pain NCPDocumento2 páginasAcute Pain NCPBobby Valencerina100% (1)
- Uterine Anomaly, Fibroid Uterus, Ovarian Tumor, Uterine ProlapseDocumento30 páginasUterine Anomaly, Fibroid Uterus, Ovarian Tumor, Uterine ProlapseVijith.V.kumar80% (5)
- IndicationDocumento70 páginasIndicationPKS 1988Ainda não há avaliações
- Information System in KimsDocumento10 páginasInformation System in KimsRoopesh KannurAinda não há avaliações
- Pancreatitis Acute - StatPearls - NCBI BookshelfDocumento6 páginasPancreatitis Acute - StatPearls - NCBI BookshelfJosé Jefferson Da SilvaAinda não há avaliações
- 21 5 Rosenfield PDFDocumento4 páginas21 5 Rosenfield PDFAbdul ZulhairuAinda não há avaliações
- Why Did You Decide To Become A NurseDocumento4 páginasWhy Did You Decide To Become A Nurseaisyah andyAinda não há avaliações
- 5z23. ED Crowding Overview and Toolkit (Dec 2015)Documento33 páginas5z23. ED Crowding Overview and Toolkit (Dec 2015)Peter 'Pierre' RobsonAinda não há avaliações
- Generic Name: Classification: IndicationDocumento2 páginasGeneric Name: Classification: IndicationKristine YoungAinda não há avaliações
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsAinda não há avaliações
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDNo EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDNota: 5 de 5 estrelas5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNo EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNota: 4 de 5 estrelas4/5 (404)
- The Age of Magical Overthinking: Notes on Modern IrrationalityNo EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityNota: 4 de 5 estrelas4/5 (32)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNota: 2 de 5 estrelas2/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNo EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNota: 4.5 de 5 estrelas4.5/5 (266)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)No EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Nota: 3 de 5 estrelas3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNo EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNota: 4.5 de 5 estrelas4.5/5 (82)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNo EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNota: 4 de 5 estrelas4/5 (4)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisNo EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisNota: 4.5 de 5 estrelas4.5/5 (42)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNo EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNota: 5 de 5 estrelas5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossNo EverandThe Obesity Code: Unlocking the Secrets of Weight LossNota: 4 de 5 estrelas4/5 (6)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesNo EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesNota: 4.5 de 5 estrelas4.5/5 (1412)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeNo EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeNota: 4.5 de 5 estrelas4.5/5 (254)
- The Marshmallow Test: Mastering Self-ControlNo EverandThe Marshmallow Test: Mastering Self-ControlNota: 4.5 de 5 estrelas4.5/5 (60)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisNo EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisNota: 5 de 5 estrelas5/5 (8)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.No EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Nota: 4.5 de 5 estrelas4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityNo EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityNota: 4 de 5 estrelas4/5 (5)
- To Explain the World: The Discovery of Modern ScienceNo EverandTo Explain the World: The Discovery of Modern ScienceNota: 3.5 de 5 estrelas3.5/5 (51)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedNo EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedNota: 4 de 5 estrelas4/5 (61)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisNo EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisNota: 3.5 de 5 estrelas3.5/5 (2)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryNo EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryNota: 4 de 5 estrelas4/5 (46)