Você também pode gostar
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- A Simplified ECG GuideDocumento4 páginasA Simplified ECG Guidejalan_z96% (25)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
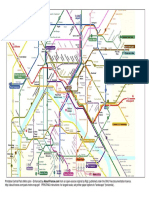
- Printable Paris Metro MapDocumento2 páginasPrintable Paris Metro MapRoisinAinda não há avaliações
- Gastrointestinal Disorders PnleDocumento23 páginasGastrointestinal Disorders Pnledelieup02100% (2)
- Brian Krumm AutopsyDocumento7 páginasBrian Krumm AutopsyMichael Cooper100% (1)
- Health Psychology 10th Edition Taylor Test BankDocumento10 páginasHealth Psychology 10th Edition Taylor Test BankJosephJohnsonfmixo100% (15)
- How I Evaluate The Neck Lymph NodesDocumento29 páginasHow I Evaluate The Neck Lymph NodesMartín Avellaneda SantoméAinda não há avaliações
- Electroconvulsive TherapyDocumento22 páginasElectroconvulsive TherapyJasmin JacobAinda não há avaliações
- ACLS DrugsDocumento16 páginasACLS Drugstostc100% (1)
- Capillary Exchange and EdemaDocumento12 páginasCapillary Exchange and EdemaSherwan R Shal100% (3)
- No Fry Fried RiceDocumento1 páginaNo Fry Fried RiceRoisinAinda não há avaliações
- Watermelon and Feta SaladDocumento1 páginaWatermelon and Feta SaladRoisinAinda não há avaliações
- Curried Potato PastiesDocumento2 páginasCurried Potato PastiesRoisinAinda não há avaliações
- Belfast PlanoDocumento2 páginasBelfast PlanoCaro DiazAinda não há avaliações
- Cardiovascular Circuit Training WorkoutDocumento1 páginaCardiovascular Circuit Training WorkoutRoisinAinda não há avaliações
- Roasted Spring Vegetables - Bless This MessDocumento2 páginasRoasted Spring Vegetables - Bless This MessRoisinAinda não há avaliações
- Versailles Palace: ParisDocumento2 páginasVersailles Palace: ParisRoisinAinda não há avaliações
- Homemade Chicken Nuggets: IngredientsDocumento2 páginasHomemade Chicken Nuggets: IngredientsRoisinAinda não há avaliações
- Mexican Restaurant-Style Cauliflower RiceDocumento2 páginasMexican Restaurant-Style Cauliflower RiceRoisinAinda não há avaliações
- Campusmap PDFDocumento2 páginasCampusmap PDFDenis DalliAinda não há avaliações
- Banana Muffins: IngredientsDocumento1 páginaBanana Muffins: IngredientsRoisinAinda não há avaliações
- Conditions of Assistance for Part Time Study & CPDDocumento2 páginasConditions of Assistance for Part Time Study & CPDRoisinAinda não há avaliações
- Exercise count-up workout trackerDocumento2 páginasExercise count-up workout trackerRoisinAinda não há avaliações
- FitnessAssessment 2015 16 PDFDocumento16 páginasFitnessAssessment 2015 16 PDFlaxave8817Ainda não há avaliações
- Leaflet Physical Activity Recommendations PDFDocumento2 páginasLeaflet Physical Activity Recommendations PDFRoisinAinda não há avaliações
- Delayed Onset Muscle Soreness (Doms)Documento2 páginasDelayed Onset Muscle Soreness (Doms)steffiecruz06Ainda não há avaliações
- Trust SoundtrackDocumento2 páginasTrust SoundtrackRoisinAinda não há avaliações
- Physical Activity and Common Mental DisordersDocumento9 páginasPhysical Activity and Common Mental DisordersRoisinAinda não há avaliações
- Folic AcidDocumento2 páginasFolic AcidRoisinAinda não há avaliações
- Trans FatsDocumento2 páginasTrans FatsRoisinAinda não há avaliações
- n55 Australian Dietary Guidelines 130530 PDFDocumento226 páginasn55 Australian Dietary Guidelines 130530 PDFtech1322Ainda não há avaliações
- Files 10624pfibrosarcomaDocumento4 páginasFiles 10624pfibrosarcomaLily NGAinda não há avaliações
- Vegetarian Food FactsDocumento2 páginasVegetarian Food FactsRoisinAinda não há avaliações
- A Guide For Exercising During and After Treatment For Cancer PDFDocumento20 páginasA Guide For Exercising During and After Treatment For Cancer PDFRoisinAinda não há avaliações
- Health & Fitness Journal: of CanadaDocumento13 páginasHealth & Fitness Journal: of CanadaRoisinAinda não há avaliações
- PregnancyDocumento2 páginasPregnancyRoisinAinda não há avaliações
- Starting An Exercise Program: Health and Medical Questionnaire Fitness Assessment Informed ConsentDocumento2 páginasStarting An Exercise Program: Health and Medical Questionnaire Fitness Assessment Informed ConsentRoisinAinda não há avaliações
- How To Work With Health Care Providers: A Systematic ApproachDocumento8 páginasHow To Work With Health Care Providers: A Systematic ApproachRoisinAinda não há avaliações
- Types of Arrhythmias and Bradycardia Treatment AlgorithmsDocumento18 páginasTypes of Arrhythmias and Bradycardia Treatment AlgorithmsZega AgustianAinda não há avaliações
- AD8232 ECG MonitoringDocumento7 páginasAD8232 ECG Monitoringsupport ubicuoAinda não há avaliações
- 2016 AHA/ACC Guideline On The Management of Patients With Lower Extremity Peripheral Artery DiseaseDocumento56 páginas2016 AHA/ACC Guideline On The Management of Patients With Lower Extremity Peripheral Artery DiseaseSilvana-Elena HojdaAinda não há avaliações
- EMT Review - Baseline Vital Signs and SAMPLE HistoryDocumento7 páginasEMT Review - Baseline Vital Signs and SAMPLE HistorymrspatmoreAinda não há avaliações
- Protocol For Intern DoctorsDocumento122 páginasProtocol For Intern DoctorsDr. BoomAinda não há avaliações
- Diseases of The Small Intestine-1Documento70 páginasDiseases of The Small Intestine-1ElvisAinda não há avaliações
- CLP 402: Pharmacotherapy of Diabetes Mellitus: David ShalkurDocumento25 páginasCLP 402: Pharmacotherapy of Diabetes Mellitus: David Shalkurbassey etoboAinda não há avaliações
- Circulation BioHackDocumento9 páginasCirculation BioHackManav SinghAinda não há avaliações
- PHYSIOLOGIC CHANGES DURING PREGNANCYDocumento4 páginasPHYSIOLOGIC CHANGES DURING PREGNANCYAdamAinda não há avaliações
- Nervous System Lesson 1Documento7 páginasNervous System Lesson 1Yennifer NivarAinda não há avaliações
- Manitou Access Platform 165 Atj Repair Manual 547343Documento22 páginasManitou Access Platform 165 Atj Repair Manual 547343kekysib100% (44)
- International Certificates Benefits of Using Anti-Radiation Mobile ChipDocumento4 páginasInternational Certificates Benefits of Using Anti-Radiation Mobile ChipSanjay GuptaAinda não há avaliações
- Revell 2014Documento6 páginasRevell 2014kemoAinda não há avaliações
- Histologyoftracheaandlung 160315034320Documento65 páginasHistologyoftracheaandlung 160315034320MUBEEN SHAIKHAinda não há avaliações
- Peripheral Artery Disease: Clinical PracticeDocumento11 páginasPeripheral Artery Disease: Clinical Practiceapi-311409998Ainda não há avaliações
- GAGAL GINJAL KRONIS DAN INDIKASI DIALISISDocumento34 páginasGAGAL GINJAL KRONIS DAN INDIKASI DIALISISDjumadi AkbarAinda não há avaliações
- The 12 Lead Ecg HandoutDocumento5 páginasThe 12 Lead Ecg HandoutReza MajidiAinda não há avaliações
- Cardiovascular SystemDocumento10 páginasCardiovascular Systemapi-283312136Ainda não há avaliações
- Heart Morphology Sea SnakeDocumento6 páginasHeart Morphology Sea SnakeduraivelanAinda não há avaliações
- Diabetic Foot Ulcer Internist ApproachDocumento57 páginasDiabetic Foot Ulcer Internist ApproachSandip DAinda não há avaliações
- 5b9f87df82236UG Syllabus (MBBS) AIIMS RaipurDocumento8 páginas5b9f87df82236UG Syllabus (MBBS) AIIMS RaipurBri MinAinda não há avaliações
- 4 EpistaxisDocumento51 páginas4 EpistaxisNicAinda não há avaliações