Você também pode gostar
- Anatomical SieveDocumento4 páginasAnatomical Sieveusmle_social_retardsAinda não há avaliações
- Clinical Exam QuestionsDocumento32 páginasClinical Exam QuestionsAtiqah ShahAinda não há avaliações
- Medicine Long CaseDocumento26 páginasMedicine Long Casewhee182Ainda não há avaliações
- Manual Lab-Act PA RPS For Student 2024Documento12 páginasManual Lab-Act PA RPS For Student 2024Jason Maxwell mcguireAinda não há avaliações
- Endometrial CarcinomaDocumento9 páginasEndometrial CarcinomatharikaneelawathuraAinda não há avaliações
- Long Case PaedDocumento21 páginasLong Case Paedwhee182Ainda não há avaliações
- Gynae KEMU Toacs StationsDocumento8 páginasGynae KEMU Toacs StationsMuhammad Aacem Khan100% (1)
- BREASTDocumento17 páginasBREASTgan choon huiAinda não há avaliações
- Oncology NursingDocumento21 páginasOncology NursingAqib SatarAinda não há avaliações
- Evolution 200 Years of Healthcare Questions HST 8-30-21Documento3 páginasEvolution 200 Years of Healthcare Questions HST 8-30-21Nasdasia AnimAinda não há avaliações
- Medicine Workshop Part IDocumento24 páginasMedicine Workshop Part Ihafsahghazali88Ainda não há avaliações
- Station 1: Health Review - FAIL: Station 2: Menstrual Dysfunction - PassDocumento17 páginasStation 1: Health Review - FAIL: Station 2: Menstrual Dysfunction - PassqurbanAinda não há avaliações
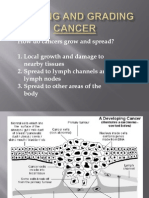
- Staging and Grading CancerDocumento20 páginasStaging and Grading CancerSillent Kaze Of FKGAinda não há avaliações
- Coventry 06.2012Documento14 páginasCoventry 06.2012karan270Ainda não há avaliações
- Preskas BedahDocumento20 páginasPreskas BedahRedhafini AzizahAinda não há avaliações
- Thyroid Ultrasound, State of The ArtDocumento15 páginasThyroid Ultrasound, State of The ArtDe DawnAinda não há avaliações
- Surgery Cases UKDocumento88 páginasSurgery Cases UKmolhamgaaferAinda não há avaliações
- Question Answer Surgery Mbbs 2nd Paper CDocumento274 páginasQuestion Answer Surgery Mbbs 2nd Paper CShivam AgarwalAinda não há avaliações
- Case Study Breast CaDocumento32 páginasCase Study Breast Caapi-391376321Ainda não há avaliações
- Congress On Cancer Calcutta Feb 1990Documento87 páginasCongress On Cancer Calcutta Feb 1990Arun Kanth100% (2)
- Case Study-Breast CADocumento11 páginasCase Study-Breast CAJoanna Cabildo83% (6)
- Surgery by HamoudDocumento89 páginasSurgery by Hamoudelhamy magdyAinda não há avaliações
- CancerDocumento84 páginasCancerKaruna KumariAinda não há avaliações
- Ilya Bafailov Rqs 12/27/2017: B. Postganglionic SympatheticDocumento3 páginasIlya Bafailov Rqs 12/27/2017: B. Postganglionic SympatheticBinayak UpadhyayaAinda não há avaliações
- A Rare Case of Paediatric Lung Tumor: Pleuropulmonary Blastoma (Type-1 PPB)Documento1 páginaA Rare Case of Paediatric Lung Tumor: Pleuropulmonary Blastoma (Type-1 PPB)Javed AliAinda não há avaliações
- LC1 Breast CaDocumento12 páginasLC1 Breast CaTony YongAinda não há avaliações
- Preskas BedahDocumento23 páginasPreskas BedahAlimuslimahAinda não há avaliações
- December 2008final FRCA VivaDocumento43 páginasDecember 2008final FRCA Vivajahangirealam100% (2)
- Cups Neck by Dr. Musaib MushtaqDocumento42 páginasCups Neck by Dr. Musaib MushtaqDr. Musaib MushtaqAinda não há avaliações
- Case Study 2Documento37 páginasCase Study 2api-391842100Ainda não há avaliações
- 2023 April SHORTS and SPOTSDocumento11 páginas2023 April SHORTS and SPOTSAdam CristaudoAinda não há avaliações
- Thyroid CancerDocumento15 páginasThyroid CancerA. Lizette PabloAinda não há avaliações
- This Study Resource Was: Nursing of Adults I Breast Cancer Case StudyDocumento3 páginasThis Study Resource Was: Nursing of Adults I Breast Cancer Case StudyJoseAinda não há avaliações
- PRO 2012 Short Case (Surgical) CompilationDocumento24 páginasPRO 2012 Short Case (Surgical) CompilationvijayaAinda não há avaliações
- PGI TangDocumento28 páginasPGI Tangjem.tangAinda não há avaliações
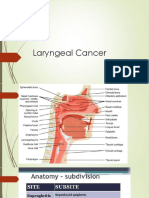
- Laryngeal Cancer 1Documento49 páginasLaryngeal Cancer 1Kpj KpjAinda não há avaliações
- Metro College of Nursing Lesson Plan: Name: Group: Venue: Date: Topic: Subject: Previous KnowledgeDocumento5 páginasMetro College of Nursing Lesson Plan: Name: Group: Venue: Date: Topic: Subject: Previous KnowledgeAvadhesh TripathiAinda não há avaliações
- EBM 2018 - Head and CancersDocumento136 páginasEBM 2018 - Head and CancersChandramohan SettyAinda não há avaliações
- 0 Yazan Mini-OSCE BreastDocumento41 páginas0 Yazan Mini-OSCE Breastmoyasserayoub78Ainda não há avaliações
- Long Case Surgery Exam QuestionDocumento25 páginasLong Case Surgery Exam Questionwhee182Ainda não há avaliações
- A Case Study In:: Thyroid CancerDocumento17 páginasA Case Study In:: Thyroid CancerJaimie La PenaAinda não há avaliações
- Oncology Handouts PDFDocumento21 páginasOncology Handouts PDFPhilip Simangan100% (1)
- A Case Study In:: Thyroid CancerDocumento18 páginasA Case Study In:: Thyroid CancerJaimie La PenaAinda não há avaliações
- Chiong - Clinical Pharmacy Breast CancerDocumento8 páginasChiong - Clinical Pharmacy Breast CancerJohn Miguel ChiongAinda não há avaliações
- Exam Osce 3Documento37 páginasExam Osce 3momo100% (1)
- Tugas RidhaDocumento8 páginasTugas RidharidhaAinda não há avaliações
- Nasopharyngeal Cancer CompleteDocumento54 páginasNasopharyngeal Cancer CompleteAmemonsajaah AmemonAinda não há avaliações
- Eng4Med Unidades 5 - 9-11-24Documento14 páginasEng4Med Unidades 5 - 9-11-24Josefa Dainery Hernandez RiveroAinda não há avaliações
- Oncology Nursing Handouts 1Documento8 páginasOncology Nursing Handouts 1pauchanmnlAinda não há avaliações
- Medical Lecture: Nazem ShamsDocumento26 páginasMedical Lecture: Nazem ShamsMahnoor AnwarAinda não há avaliações
- Cell Ab ActivitiesDocumento7 páginasCell Ab ActivitiesJanelle Cabida Supnad100% (1)
- CASE ANALYSIS - Nasopharyngeal CancerDocumento8 páginasCASE ANALYSIS - Nasopharyngeal CancerTerry Mae Atilazal SarciaAinda não há avaliações
- Diagnosis of Cancer: 2-Biochemical AssaysDocumento22 páginasDiagnosis of Cancer: 2-Biochemical AssaysSawsan Z. JwaiedAinda não há avaliações
- All You Have Ever Wanted To Know About Mucoepidermoid CarcinomaDocumento63 páginasAll You Have Ever Wanted To Know About Mucoepidermoid CarcinomaNeeraj TekariaAinda não há avaliações
- ONCOLOGYDocumento6 páginasONCOLOGYRizMarie100% (2)
- Pancoast Syndrome, (Apical Lung Cancer) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandPancoast Syndrome, (Apical Lung Cancer) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- Essentials of Radiofrequency Ablation of the Spine and JointsNo EverandEssentials of Radiofrequency Ablation of the Spine and JointsAinda não há avaliações
- Contribution Of Ultrasound To Inflammatory Abdominal DiseaseNo EverandContribution Of Ultrasound To Inflammatory Abdominal DiseaseAinda não há avaliações
- Multiple Choice Questions in Clinical Radiology: For Medical Practitioners and Medical StudentsNo EverandMultiple Choice Questions in Clinical Radiology: For Medical Practitioners and Medical StudentsNota: 5 de 5 estrelas5/5 (1)
- Inguinal Scrotal SwellingsDocumento23 páginasInguinal Scrotal SwellingsAzmyza Azmy100% (1)
- Revision Microbiology - EditedDocumento14 páginasRevision Microbiology - EditedAzmyza AzmyAinda não há avaliações
- Emj Cases : Questions For Case 1Documento8 páginasEmj Cases : Questions For Case 1Azmyza Azmy100% (1)
- Combined 2 or More DMARDS Is More Effective Than MonotherapyDocumento7 páginasCombined 2 or More DMARDS Is More Effective Than MonotherapyAzmyza AzmyAinda não há avaliações
- 222Documento7 páginas222Erl DrizAinda não há avaliações
- 1 Revised Food Borne Illness Lecture 1Documento5 páginas1 Revised Food Borne Illness Lecture 1Tarequl Islam NishadAinda não há avaliações
- C I Care Badge CardsDocumento1 páginaC I Care Badge CardsMai MaiAinda não há avaliações
- Literature & MedicineDocumento14 páginasLiterature & MedicineJoyce LeungAinda não há avaliações
- 6 - Toronto Notes 2011 - DermatologyDocumento46 páginas6 - Toronto Notes 2011 - DermatologyqobsarAinda não há avaliações
- Acceptable Prescribing Terms and Abbreviations PosterDocumento1 páginaAcceptable Prescribing Terms and Abbreviations PosterAdelAinda não há avaliações
- National Guidelines For The Use of Complementary Therapies in Supportive and Palliative CareDocumento112 páginasNational Guidelines For The Use of Complementary Therapies in Supportive and Palliative Caredorothywyn50% (2)
- Dermatomycological Profile of Patients in A Tertiary Care Hospital of Western MaharashtraDocumento2 páginasDermatomycological Profile of Patients in A Tertiary Care Hospital of Western MaharashtraApple IdeaAinda não há avaliações
- Vitamin D3Documento29 páginasVitamin D3Ambreen AmirAinda não há avaliações
- Project in Mapeh (Health)Documento8 páginasProject in Mapeh (Health)guache warrinAinda não há avaliações
- AJACM 2010 5 2 Wang Juyi Interview Part 1 of 2 - LiuDocumento7 páginasAJACM 2010 5 2 Wang Juyi Interview Part 1 of 2 - LiuYagtaliAinda não há avaliações
- Femoral Block Vs Adductor Canal Block: Regional Analgesia For Total Knee ArthroplastyDocumento10 páginasFemoral Block Vs Adductor Canal Block: Regional Analgesia For Total Knee ArthroplastyStanford AnesthesiaAinda não há avaliações
- Jurnal Manajemen Apotek PDFDocumento11 páginasJurnal Manajemen Apotek PDFAlexSiNagaAinda não há avaliações
- Congenital Postero-Medial Bowing of The Tibia and Fibula: Is Early Surgery Worthwhile?Documento8 páginasCongenital Postero-Medial Bowing of The Tibia and Fibula: Is Early Surgery Worthwhile?Kaustubh KeskarAinda não há avaliações
- Caffeine Intoxication Consumer MonographDocumento3 páginasCaffeine Intoxication Consumer MonographEfdio Manuel Joshiro SiagianAinda não há avaliações
- Jurnal Daun Jati Cina Senna AlexandriaDocumento7 páginasJurnal Daun Jati Cina Senna AlexandriaFransLei Vadoel SaelAinda não há avaliações
- Rev Plans For 20eb0110 - Provincial HospitalDocumento20 páginasRev Plans For 20eb0110 - Provincial HospitalElvin AsanasAinda não há avaliações
- Medi Assist Policy Conditions 2018-19Documento22 páginasMedi Assist Policy Conditions 2018-19saran2rasuAinda não há avaliações
- The Science of SingingDocumento18 páginasThe Science of SingingK100% (2)
- Pathophysiology Schematic Diagram and NarrativeDocumento15 páginasPathophysiology Schematic Diagram and NarrativeKathrina CraveAinda não há avaliações
- Internship 1 4Documento75 páginasInternship 1 4Mariah Sharmane Juego Santos100% (2)
- Fever in Children With ChemoteraphyDocumento23 páginasFever in Children With ChemoteraphyImanuel Far-FarAinda não há avaliações
- Rajiv Gandhi University of Health Sciences, Karnataka, BangaloreDocumento27 páginasRajiv Gandhi University of Health Sciences, Karnataka, BangaloreJyotiAinda não há avaliações
- 07 The Molecular Biology of CancerDocumento39 páginas07 The Molecular Biology of CancerJustin GonzalesAinda não há avaliações
- Perioperative Care For CABG PatientsDocumento32 páginasPerioperative Care For CABG PatientsAya EyadAinda não há avaliações
- Jurnal - Komponen DarahDocumento6 páginasJurnal - Komponen Darahvivi maykasariAinda não há avaliações
- Spiritual Healing As An Alternative Health Care Delivery in Benue State Issues and ChallengesDocumento11 páginasSpiritual Healing As An Alternative Health Care Delivery in Benue State Issues and ChallengesEditor IJTSRDAinda não há avaliações
- Bonitas 2023 Network ListDocumento33 páginasBonitas 2023 Network ListStéfan RoodtAinda não há avaliações
- Common Emergency DrugsDocumento61 páginasCommon Emergency DrugsFebee Gee100% (1)
- PDF Book UrduDocumento4 páginasPDF Book UrduMuhammad KamranAinda não há avaliações