Você também pode gostar
- Cardiac Electrophysiology Without FluoroscopyNo EverandCardiac Electrophysiology Without FluoroscopyRiccardo ProiettiAinda não há avaliações
- Biomedical Signal Processing and Control: Changchen Zhao, Chun-Liang Lin, Weihai Chen, Ming-Kun Chen, Jianhua WangDocumento10 páginasBiomedical Signal Processing and Control: Changchen Zhao, Chun-Liang Lin, Weihai Chen, Ming-Kun Chen, Jianhua WangAdi Muhammad QuddusAinda não há avaliações
- Classification of Gait Phases From Lower Limb EMG: Application To Exoskeleton OrthosisDocumento4 páginasClassification of Gait Phases From Lower Limb EMG: Application To Exoskeleton OrthosisshravantataAinda não há avaliações
- An Integrated Fall Prevention System With Single-Channel EEG and EMG SensorDocumento7 páginasAn Integrated Fall Prevention System With Single-Channel EEG and EMG SensorNG Jun HowAinda não há avaliações
- Design and Development of A Portable Recording System For Simultaneous Acquisition of SCG and ECG SignalsDocumento6 páginasDesign and Development of A Portable Recording System For Simultaneous Acquisition of SCG and ECG SignalsSyed Shouvik Islam (sSi)Ainda não há avaliações
- Oe 30 8 13121 DNN ShuyangDocumento13 páginasOe 30 8 13121 DNN Shuyangpuma flyerAinda não há avaliações
- Development of A Smart Garment For The Assessment of Cardiac Mechanical Performance and Other Vital Signs During Sleep in MicrogravityDocumento9 páginasDevelopment of A Smart Garment For The Assessment of Cardiac Mechanical Performance and Other Vital Signs During Sleep in MicrogravitynarykAinda não há avaliações
- 27 Feature Extraction and Classifier in The Development of Exoskeleton Based On Emg Signal Control A ReviewDocumento7 páginas27 Feature Extraction and Classifier in The Development of Exoskeleton Based On Emg Signal Control A ReviewTriwiyanto TriwiyantoAinda não há avaliações
- Nazmi 2015Documento6 páginasNazmi 2015u5600291Ainda não há avaliações
- Wearable Sensors For Gait AnalysisDocumento5 páginasWearable Sensors For Gait AnalysissanahujalidiaAinda não há avaliações
- Document PDFDocumento5 páginasDocument PDFbella kAinda não há avaliações
- 11 MagIC System A New Textile-Based Wearable Device For Biological Signal Monitoring. Applicability in Daily Life and Clinical Setting.Documento3 páginas11 MagIC System A New Textile-Based Wearable Device For Biological Signal Monitoring. Applicability in Daily Life and Clinical Setting.narykAinda não há avaliações
- Smart Clothes With Bio-Sensors For ECG Monitoring: P.Sakthi Shunmuga Sundaram, N.Hari Basker, L.NatrayanDocumento4 páginasSmart Clothes With Bio-Sensors For ECG Monitoring: P.Sakthi Shunmuga Sundaram, N.Hari Basker, L.NatrayanazmiAinda não há avaliações
- Paper1 IJCET 2015Documento5 páginasPaper1 IJCET 2015Retheep RajAinda não há avaliações
- QRS Detection Based On An Advanced Multilevel AlgorithmDocumento8 páginasQRS Detection Based On An Advanced Multilevel AlgorithmOussama El B'charriAinda não há avaliações
- Transition Detection in Body Movement Activities For Wearable ECGDocumento4 páginasTransition Detection in Body Movement Activities For Wearable ECGAlex WongAinda não há avaliações
- Morais 2021 J. Phys. Conf. Ser. 1826 012084Documento8 páginasMorais 2021 J. Phys. Conf. Ser. 1826 012084Johnny Joe AguilarAinda não há avaliações
- Literature Review: 2.1 A Survey of Modern Wearable ECG Recording and Monitoring SystemsDocumento12 páginasLiterature Review: 2.1 A Survey of Modern Wearable ECG Recording and Monitoring SystemsNarayanamoorthyAinda não há avaliações
- Development of 2-DOF Powered Exoskeleton For Upper Limb RehabilitationDocumento2 páginasDevelopment of 2-DOF Powered Exoskeleton For Upper Limb RehabilitationWarnithaAinda não há avaliações
- Article 4Documento10 páginasArticle 4Tri WiyantoAinda não há avaliações
- Emg Load v6 Sumair Submit Version ResearchGateDocumento9 páginasEmg Load v6 Sumair Submit Version ResearchGatePopescu ValiAinda não há avaliações
- Evaluation of Data Compression Methods For Efficient Transport and Classification of Facial Emg SignalsDocumento21 páginasEvaluation of Data Compression Methods For Efficient Transport and Classification of Facial Emg Signalsbizhan abgarmiAinda não há avaliações
- Systematic Design and HRV Analysis of A Portable ECG System Using Arduino and LabVIEW For Biomedical Engineering TrainingDocumento11 páginasSystematic Design and HRV Analysis of A Portable ECG System Using Arduino and LabVIEW For Biomedical Engineering Trainingsantosra211216Ainda não há avaliações
- Analysis of Myoelectric Signals To Prosthesis ApplicationsDocumento8 páginasAnalysis of Myoelectric Signals To Prosthesis ApplicationsBrunaAinda não há avaliações
- Cardiovascular Measurement SystemDocumento8 páginasCardiovascular Measurement Systemजैत्र YadavAinda não há avaliações
- Fariha 2020 J. Phys. Conf. Ser. 1532 012022Documento12 páginasFariha 2020 J. Phys. Conf. Ser. 1532 012022Anagha PradeepAinda não há avaliações
- 4 PBDocumento12 páginas4 PBkhouloud pfeAinda não há avaliações
- ECG QRS Complex DetectorDocumento6 páginasECG QRS Complex DetectorIjsrnet EditorialAinda não há avaliações
- Signal Condition and Acquisition System For A Low Cost EMG Based Prosthetic HandDocumento9 páginasSignal Condition and Acquisition System For A Low Cost EMG Based Prosthetic HandNazhan HakeemAinda não há avaliações
- Upper Limb Muscle Fatigue Analysis Using Multi-Channel Surface EMGDocumento5 páginasUpper Limb Muscle Fatigue Analysis Using Multi-Channel Surface EMGMuhammad Fauzi D4 ElektromedikAinda não há avaliações
- Comparing Feature-Based Classifiers and Convolutional Neural Networks To Detect Arrhythmia From Short Segments of ECGDocumento4 páginasComparing Feature-Based Classifiers and Convolutional Neural Networks To Detect Arrhythmia From Short Segments of ECGMhd rdbAinda não há avaliações
- International Journal of Engineering Research and DevelopmentDocumento11 páginasInternational Journal of Engineering Research and DevelopmentIJERDAinda não há avaliações
- Elbow Flexion and Extension Identification Using Surface Electromyography SignalsDocumento5 páginasElbow Flexion and Extension Identification Using Surface Electromyography SignalsAlexandra Torres GacharnaAinda não há avaliações
- 0.6 mm的最小分辨率滑动栅格Documento11 páginas0.6 mm的最小分辨率滑动栅格123Ainda não há avaliações
- Computers in Biology and Medicine: SciencedirectDocumento12 páginasComputers in Biology and Medicine: SciencedirectYasser HamedAinda não há avaliações
- Robust Classification of Cardiac Arrhythmia Using Machine LearningDocumento9 páginasRobust Classification of Cardiac Arrhythmia Using Machine LearningIJRASETPublicationsAinda não há avaliações
- Automated QRS Detection Using Empirical Mode Decomposition and K-MeansDocumento8 páginasAutomated QRS Detection Using Empirical Mode Decomposition and K-MeansInternational Journal of Innovative Science and Research TechnologyAinda não há avaliações
- Leicht, Lennart-1017-A Safaty Belt Integrated Sensor Syistem For Heart Activity and RespirationDocumento5 páginasLeicht, Lennart-1017-A Safaty Belt Integrated Sensor Syistem For Heart Activity and RespirationArda Safira Kardono D4AJAinda não há avaliações
- Comparative Analysis of Machine Learning Algorithms On Myoelectric Signal From Intact and Transradial Amputated LimbsDocumento9 páginasComparative Analysis of Machine Learning Algorithms On Myoelectric Signal From Intact and Transradial Amputated LimbsIAES IJAIAinda não há avaliações
- FPGA-based System For Heart Rate Monitoring PDFDocumento12 páginasFPGA-based System For Heart Rate Monitoring PDFkishorechiyaAinda não há avaliações
- 1 s2.0 S093336572200001X MainDocumento11 páginas1 s2.0 S093336572200001X MainNaila AshrafAinda não há avaliações
- Acquisition and Analysis of EMG Signals To Recognize Multiple Hand Movements For Prosthetic ApplicationsDocumento12 páginasAcquisition and Analysis of EMG Signals To Recognize Multiple Hand Movements For Prosthetic ApplicationsEdgarGonzálezAinda não há avaliações
- Development and Evaluation of One Arm Electrode BasedDocumento4 páginasDevelopment and Evaluation of One Arm Electrode BasedKarthik Raj VAinda não há avaliações
- Research Article: An Effective LSTM Recurrent Network To Detect Arrhythmia On Imbalanced ECG DatasetDocumento11 páginasResearch Article: An Effective LSTM Recurrent Network To Detect Arrhythmia On Imbalanced ECG DatasettestAinda não há avaliações
- ECG Compression and Labview Implementation: Tatiparti Padma, M. Madhavi Latha, Abrar AhmedDocumento7 páginasECG Compression and Labview Implementation: Tatiparti Padma, M. Madhavi Latha, Abrar AhmedManjot AroraAinda não há avaliações
- Semantic ECG Interval Segmentation Using AutoencodersDocumento7 páginasSemantic ECG Interval Segmentation Using AutoencodersMhd rdbAinda não há avaliações
- Grasp Recognition From Myoelectric Signals: Simon Ferguson G Reg DunlopDocumento5 páginasGrasp Recognition From Myoelectric Signals: Simon Ferguson G Reg Dunlopwmp8611024213Ainda não há avaliações
- Wireless Sensor Module For 3-Axis Vibration and Tilt Monitoring On The Structural BuildingDocumento8 páginasWireless Sensor Module For 3-Axis Vibration and Tilt Monitoring On The Structural BuildingDimas SuryaAinda não há avaliações
- Laboratory Manual: 18EC3017 Biomedical Electronics & IOT For HealthcareDocumento16 páginasLaboratory Manual: 18EC3017 Biomedical Electronics & IOT For HealthcareSatya GopalAinda não há avaliações
- Automation of ECG Heart Beat Detection Using Morphological Filtering and Daubechies Wavelet TransformDocumento6 páginasAutomation of ECG Heart Beat Detection Using Morphological Filtering and Daubechies Wavelet TransformIOSRJEN : hard copy, certificates, Call for Papers 2013, publishing of journalAinda não há avaliações
- Wearable Gait MeasurementDocumento4 páginasWearable Gait MeasurementHasballah ZakariaAinda não há avaliações
- Automatic Classification of Heartbeats Using Wavelet Neural NetworkDocumento11 páginasAutomatic Classification of Heartbeats Using Wavelet Neural NetworkSamir GhoualiAinda não há avaliações
- Electronic Infosystems: By: Witkorio Penkorio Armani Wieluneiro Wyspiacze Sowissimo SopelliniDocumento30 páginasElectronic Infosystems: By: Witkorio Penkorio Armani Wieluneiro Wyspiacze Sowissimo SopelliniPrzemysław TarkowskiAinda não há avaliações
- Gesture Recognition Based On Nano-Gold Flexible Sensor UsingDocumento6 páginasGesture Recognition Based On Nano-Gold Flexible Sensor UsingChristian F. VegaAinda não há avaliações
- Comparison of Accelerometer-Based Energy Expenditure Estimation AlgorithmsDocumento8 páginasComparison of Accelerometer-Based Energy Expenditure Estimation AlgorithmsSergio Raposo PerezAinda não há avaliações
- Portable EMG Data Acquisition Module For Upper Limb Prosthesis ApplicationDocumento8 páginasPortable EMG Data Acquisition Module For Upper Limb Prosthesis ApplicationHoàng ThắngAinda não há avaliações
- ةزـــــــــغ - رــــهزلأا ةعماج Al Azhar University - GazaDocumento18 páginasةزـــــــــغ - رــــهزلأا ةعماج Al Azhar University - GazaAhmad Ali KhaderAinda não há avaliações
- Electromyography (EMG) Based Control For Shoulder Muscles: Long Doan Thanh, Nhon Phan Nguyen QuyDocumento5 páginasElectromyography (EMG) Based Control For Shoulder Muscles: Long Doan Thanh, Nhon Phan Nguyen QuyPhan Nguyễn Quy NhơnAinda não há avaliações
- Patient Adaptive ECG Beat Classifier Using Repetition Detection Approach Enhanced by Neural NetworksDocumento5 páginasPatient Adaptive ECG Beat Classifier Using Repetition Detection Approach Enhanced by Neural NetworksHạt DẻAinda não há avaliações
- DWT PDFDocumento7 páginasDWT PDFsumanth_0678Ainda não há avaliações
- Circuitos Sujetadores Con DiodosDocumento50 páginasCircuitos Sujetadores Con DiodosrobertoAinda não há avaliações
- MEM ActuadoresDocumento62 páginasMEM ActuadoresrobertoAinda não há avaliações
- CH 05 Emisor Comun BJTDocumento16 páginasCH 05 Emisor Comun BJTrobertoAinda não há avaliações
- Opportunities For Collaboration With IBM: Allen MalonyDocumento44 páginasOpportunities For Collaboration With IBM: Allen MalonyrobertoAinda não há avaliações
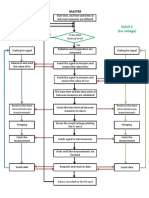
- Flow Chart PVDocumento1 páginaFlow Chart PVrobertoAinda não há avaliações
- Car Ignition With IgbtsDocumento9 páginasCar Ignition With IgbtsrobertoAinda não há avaliações
- CaptoprilDocumento2 páginasCaptoprilJohn Louie EscardaAinda não há avaliações
- Mechanical VentilationDocumento16 páginasMechanical VentilationArt Christian Ramos88% (8)
- HPLC 09 2014Documento29 páginasHPLC 09 2014api-243480627Ainda não há avaliações
- Qbank FormatDocumento5 páginasQbank FormatpashaAinda não há avaliações
- Physical Assessment Vital SignsDocumento17 páginasPhysical Assessment Vital SignsArvi GayeAinda não há avaliações
- Big Book of Kaiju #0Documento17 páginasBig Book of Kaiju #0Boracchio Pasquale100% (1)
- Pelvic Floor MuscleDocumento11 páginasPelvic Floor MuscleSonia guptaAinda não há avaliações
- Quiz-4-Storage Mechanisms and Control in Carbohydrate MetabolismDocumento5 páginasQuiz-4-Storage Mechanisms and Control in Carbohydrate Metabolismaichiii.bearAinda não há avaliações
- Antigen & AntibodiesDocumento16 páginasAntigen & AntibodiesYing Ming TangAinda não há avaliações
- Background Results: DR Aditya Bhat, DR, Amit Misri Department of Paediatric Cardiology, Medanta-The Medicity, GurgaonDocumento1 páginaBackground Results: DR Aditya Bhat, DR, Amit Misri Department of Paediatric Cardiology, Medanta-The Medicity, GurgaonADAinda não há avaliações
- Sturge-Weber Syndrome. Study of 55 PatientsDocumento7 páginasSturge-Weber Syndrome. Study of 55 PatientsdzhzrnAinda não há avaliações
- Write Up TutorialDocumento22 páginasWrite Up Tutorialballer0417100% (1)
- An Are Rob I C DegradationDocumento18 páginasAn Are Rob I C DegradationMartuchis EstradaAinda não há avaliações
- Nursing Care Plan - Mam EkaDocumento7 páginasNursing Care Plan - Mam EkaGlenn Asuncion PagaduanAinda não há avaliações
- AsthmaDocumento55 páginasAsthmaAlessandra CruzAinda não há avaliações
- FLCCC Alliance I RECOVER Management Protocol For Long Haul COVID 19 SyndromeDocumento3 páginasFLCCC Alliance I RECOVER Management Protocol For Long Haul COVID 19 SyndromeAizaz ul HaqAinda não há avaliações
- Pupillary Light ReflexDocumento2 páginasPupillary Light ReflexJohn OsborneAinda não há avaliações
- ISC Class 11 Bio Specimen PaperDocumento6 páginasISC Class 11 Bio Specimen PaperparamAinda não há avaliações
- Bsczo 102 PDFDocumento209 páginasBsczo 102 PDFajitha ajithAinda não há avaliações
- Exp 1 Group 8 MT3 ADocumento12 páginasExp 1 Group 8 MT3 AJoanna RamosoAinda não há avaliações
- DMLT I IiDocumento11 páginasDMLT I IisyedzahidshabirAinda não há avaliações
- Abdominal DistensionDocumento10 páginasAbdominal DistensionMorad ImadAinda não há avaliações
- Enteric Nervous SystemDocumento12 páginasEnteric Nervous SystemedgarAinda não há avaliações
- AP1 Lab4 Intro To Skeleton FA2021Documento15 páginasAP1 Lab4 Intro To Skeleton FA2021Kim VenturaAinda não há avaliações
- ADR Common Drug - Induced Organ DisordersDocumento45 páginasADR Common Drug - Induced Organ Disorders0009439Ainda não há avaliações
- Unlocking The BrainDocumento3 páginasUnlocking The BrainPsychedelicBaronAinda não há avaliações
- Specialization of Cerebral Hemispheres in Humans: December 2013Documento9 páginasSpecialization of Cerebral Hemispheres in Humans: December 2013Huy NgoAinda não há avaliações
- Caffeine and Primary (Migraine) Headaches-Friend or Foe?: Karl B. Alstadhaug and Anna P. AndreouDocumento13 páginasCaffeine and Primary (Migraine) Headaches-Friend or Foe?: Karl B. Alstadhaug and Anna P. AndreouPutri SantriAinda não há avaliações
- Anatomy & Physiology of Olfactory System.Documento27 páginasAnatomy & Physiology of Olfactory System.Prasanna DattaAinda não há avaliações
- Different Approaches in Pharmacological ResearchDocumento3 páginasDifferent Approaches in Pharmacological ResearcharcherselevatorsAinda não há avaliações
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)No EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Nota: 3 de 5 estrelas3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNo EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNota: 4 de 5 estrelas4/5 (404)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsAinda não há avaliações
- The Age of Magical Overthinking: Notes on Modern IrrationalityNo EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityNota: 4 de 5 estrelas4/5 (32)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisNo EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisNota: 4.5 de 5 estrelas4.5/5 (42)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDNo EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDNota: 5 de 5 estrelas5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNota: 2 de 5 estrelas2/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNo EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNota: 4.5 de 5 estrelas4.5/5 (82)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryNo EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryNota: 4 de 5 estrelas4/5 (46)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNo EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNo EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNota: 4 de 5 estrelas4/5 (4)
- The Obesity Code: Unlocking the Secrets of Weight LossNo EverandThe Obesity Code: Unlocking the Secrets of Weight LossNota: 4 de 5 estrelas4/5 (6)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesNo EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesNota: 4.5 de 5 estrelas4.5/5 (1412)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNo EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNota: 5 de 5 estrelas5/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.No EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Nota: 4.5 de 5 estrelas4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityNo EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityNota: 4 de 5 estrelas4/5 (5)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsNo EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsNota: 4.5 de 5 estrelas4.5/5 (170)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisNo EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisNota: 5 de 5 estrelas5/5 (8)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisNo EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisNota: 3.5 de 5 estrelas3.5/5 (2)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessNo EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessNota: 4.5 de 5 estrelas4.5/5 (328)
- Troubled: A Memoir of Foster Care, Family, and Social ClassNo EverandTroubled: A Memoir of Foster Care, Family, and Social ClassNota: 4.5 de 5 estrelas4.5/5 (27)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingNo EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingNota: 4 de 5 estrelas4/5 (1138)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeNo EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeNota: 4.5 de 5 estrelas4.5/5 (254)