Você também pode gostar
- Los Inicios de La Iglesia CristianaDocumento2 páginasLos Inicios de La Iglesia CristianaBaritana100% (2)
- Métodos de Exploración Psicológica II - Guia de Estudio 1Documento42 páginasMétodos de Exploración Psicológica II - Guia de Estudio 1Baritana100% (2)
- Fundaspie Aragua - Planificación de La JornadaDocumento4 páginasFundaspie Aragua - Planificación de La JornadaBaritanaAinda não há avaliações
- Conductas AdictivasDocumento5 páginasConductas AdictivasBaritanaAinda não há avaliações
- Tipos de TestDocumento22 páginasTipos de TestBaritanaAinda não há avaliações
- Psicopatología de La Atención - Resumen de ClaseDocumento4 páginasPsicopatología de La Atención - Resumen de ClaseBaritanaAinda não há avaliações
- Psicología Experimental - Teoría y Método Arnau Taller 1Documento4 páginasPsicología Experimental - Teoría y Método Arnau Taller 1BaritanaAinda não há avaliações
- Trabajo Final - Test Del Reloj y MinimentalDocumento19 páginasTrabajo Final - Test Del Reloj y MinimentalBaritana100% (1)
- Control Del Esfínter Vesical (Nocturno)Documento2 páginasControl Del Esfínter Vesical (Nocturno)BaritanaAinda não há avaliações
- PSICOPATOLOGÍA - Primer ExamenDocumento6 páginasPSICOPATOLOGÍA - Primer ExamenBaritanaAinda não há avaliações
- PSICOPATOLOGÍA - Primer ExamenDocumento6 páginasPSICOPATOLOGÍA - Primer ExamenBaritanaAinda não há avaliações
- Trastorno Del Lenguaje - Resumen de ClaseDocumento3 páginasTrastorno Del Lenguaje - Resumen de ClaseBaritanaAinda não há avaliações
- Psicopatología de La Atención - Resumen de ClaseDocumento4 páginasPsicopatología de La Atención - Resumen de ClaseBaritanaAinda não há avaliações
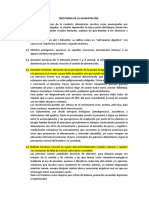
- Trastorno de La Alimentación - Resumen de ClaseDocumento2 páginasTrastorno de La Alimentación - Resumen de ClaseBaritanaAinda não há avaliações
- Orientacion - Clase 3Documento11 páginasOrientacion - Clase 3BaritanaAinda não há avaliações
- Clase de Sensopercepcion PSICOPATOLOGIADocumento10 páginasClase de Sensopercepcion PSICOPATOLOGIABaritanaAinda não há avaliações
- Bases Del Concurso de Danza UltimoDocumento11 páginasBases Del Concurso de Danza UltimoSebastian Rodrigo Loyola AraujoAinda não há avaliações
- Hta Aspectos y DirectricesDocumento22 páginasHta Aspectos y DirectricesBryan UquillasAinda não há avaliações
- CB Educacion Artistica PDFDocumento14 páginasCB Educacion Artistica PDFnuevo almacenamientoAinda não há avaliações
- DENGUE Nuevo 2 Diseño Metodologico-1Documento13 páginasDENGUE Nuevo 2 Diseño Metodologico-1Jose Luis Guaman EspinozaAinda não há avaliações
- Sesiones de Buen Trato PrimariaDocumento6 páginasSesiones de Buen Trato PrimariaJesus Manuel Trujillo AgueroAinda não há avaliações
- Donde Se Descompone La Cola de Los Burros.Documento23 páginasDonde Se Descompone La Cola de Los Burros.Carolina RodriguezAinda não há avaliações
- Actividad 3 Validacion y Confiabilidad de Los InstrumentosDocumento57 páginasActividad 3 Validacion y Confiabilidad de Los Instrumentosmonalz2412Ainda não há avaliações
- Modelo Curricular en MéxicoDocumento5 páginasModelo Curricular en MéxicoLuiz PazkualAinda não há avaliações
- Taller 2 de Diseño de ExperimentosDocumento2 páginasTaller 2 de Diseño de ExperimentosquedolimpioAinda não há avaliações
- Los Borg CUADERNO DE BITACORADocumento10 páginasLos Borg CUADERNO DE BITACORALeo RuvAinda não há avaliações
- Cadenas TróficasDocumento4 páginasCadenas TróficasLeonardo PichardoAinda não há avaliações
- Puntos Extra 2 AutocalificableDocumento4 páginasPuntos Extra 2 AutocalificableWilliam Efrén Alvarez Carmona0% (2)
- Historia Clinica Basado en OftalmologiaDocumento5 páginasHistoria Clinica Basado en Oftalmologiapolydjainer princeAinda não há avaliações
- Cod ConvolucionalesDocumento8 páginasCod ConvolucionalesMiriam Elizabeth Mora ArteagaAinda não há avaliações
- José Ortega y Gasset: Filosof IaDocumento40 páginasJosé Ortega y Gasset: Filosof IaCristian ReyesAinda não há avaliações
- Criminología Clínica e Incidencia de Orientaciones Biologicistas - Nota 10 PDFDocumento4 páginasCriminología Clínica e Incidencia de Orientaciones Biologicistas - Nota 10 PDFCelia GonzálezAinda não há avaliações
- En El Cuerpo Humano Existen 208 HuesosDocumento3 páginasEn El Cuerpo Humano Existen 208 HuesosConny EpuntoCeAinda não há avaliações
- Gema Acordes - Los DandysDocumento2 páginasGema Acordes - Los DandysMax Andrew100% (1)
- Miguel Bonilla Lopez PonenciaDocumento21 páginasMiguel Bonilla Lopez PonenciaVictorHugoSerranoMoralesAinda não há avaliações
- Presentación Sin TítuloDocumento2 páginasPresentación Sin TítuloAriadna BastidasAinda não há avaliações
- Oracle Developer Form BuilderDocumento40 páginasOracle Developer Form BuilderRaidenzAinda não há avaliações
- Soluciones de La Relación de Muestreo EstratificadoDocumento11 páginasSoluciones de La Relación de Muestreo EstratificadoDenís ChicoAinda não há avaliações
- Modelo de Análisis de Un PoemaDocumento5 páginasModelo de Análisis de Un Poemacamilo fernandezAinda não há avaliações
- Acta de Instruccion No. 007. Derechos Huamnos y CorrupcionDocumento5 páginasActa de Instruccion No. 007. Derechos Huamnos y CorrupcionquirozppclaudiaAinda não há avaliações
- Flexiòn BiaxialDocumento20 páginasFlexiòn BiaxialIsaac QuevedoAinda não há avaliações
- Actividad Virtual 9 (Grupal) GRUPO 7Documento4 páginasActividad Virtual 9 (Grupal) GRUPO 7MARIAFE JEISY VILLANUEVA URDANEGUIAinda não há avaliações
- EPIDEMIOLOGIADocumento24 páginasEPIDEMIOLOGIAJorge Emmanuel CepedaAinda não há avaliações
- PARAFILIASDocumento14 páginasPARAFILIASVíctor Valentín Fernández0% (1)
- Reporte Grupal JominyDocumento19 páginasReporte Grupal JominyCésar VenegasAinda não há avaliações
- Diccionario Biografico Italo ArgentinoDocumento65 páginasDiccionario Biografico Italo ArgentinoEsteban BekermanAinda não há avaliações