Você também pode gostar
- Cardiac CycleDocumento2 páginasCardiac CycleBilly Shan LastKagerooboroAinda não há avaliações
- ID Angka Kejadian Fraktur Mandibula Berdasa PDFDocumento14 páginasID Angka Kejadian Fraktur Mandibula Berdasa PDFBilly Shan LastKagerooboroAinda não há avaliações
- Abuse GlobalDocumento5 páginasAbuse GlobalBilly Shan LastKagerooboroAinda não há avaliações
- Disertasi Meningioma-Sex HormonDocumento143 páginasDisertasi Meningioma-Sex HormonBilly Shan LastKagerooboroAinda não há avaliações
- Chronic Otitis Externa 20060425Documento55 páginasChronic Otitis Externa 20060425ndutyyyAinda não há avaliações
- Rhamnolipid Biosurfactants As New Players in Animal and Plant Defense Against MicrobesDocumento14 páginasRhamnolipid Biosurfactants As New Players in Animal and Plant Defense Against MicrobesBilly Shan LastKagerooboroAinda não há avaliações
- DerTraChiMed Exc PDFDocumento18 páginasDerTraChiMed Exc PDFEvy Afrianti DariseAinda não há avaliações
- ID Angka Kejadian Fraktur Mandibula Berdasa PDFDocumento14 páginasID Angka Kejadian Fraktur Mandibula Berdasa PDFBilly Shan LastKagerooboroAinda não há avaliações
- Rhamnolipid Biosurfactants As New Players in Animal and Plant Defense Against MicrobesDocumento14 páginasRhamnolipid Biosurfactants As New Players in Animal and Plant Defense Against MicrobesBilly Shan LastKagerooboroAinda não há avaliações
- Oxygen or Cooling, To Make A Decision After Acute IschemiaDocumento6 páginasOxygen or Cooling, To Make A Decision After Acute IschemiaBilly Shan LastKagerooboroAinda não há avaliações
- 573 1108 1 SMDocumento6 páginas573 1108 1 SMfajar abroriAinda não há avaliações
- 573 1108 1 SMDocumento6 páginas573 1108 1 SMfajar abroriAinda não há avaliações
- Lirik Aber OMDocumento13 páginasLirik Aber OMBilly Shan LastKagerooboroAinda não há avaliações
- TH e Relation of Hyperbaric OxygenDocumento6 páginasTH e Relation of Hyperbaric OxygenBilly Shan LastKagerooboroAinda não há avaliações
- Age-Associated Resident Memory CD8 TDocumento14 páginasAge-Associated Resident Memory CD8 TBilly Shan LastKagerooboroAinda não há avaliações
- DHF Menurut WHO 2011Documento212 páginasDHF Menurut WHO 2011Jamal SutrisnaAinda não há avaliações
- The Paradox of Treg RoleDocumento8 páginasThe Paradox of Treg RoleBilly Shan LastKagerooboroAinda não há avaliações
- Wellington ICU Drug Manual v2013Documento442 páginasWellington ICU Drug Manual v2013Billy Shan LastKagerooboroAinda não há avaliações
- Endogenous IFN-β Signaling ExertsDocumento18 páginasEndogenous IFN-β Signaling ExertsBilly Shan LastKagerooboroAinda não há avaliações
- Does Normobaric Hyperoxia IncreaseDocumento8 páginasDoes Normobaric Hyperoxia IncreaseBilly Shan LastKagerooboroAinda não há avaliações
- Lirik ThirdDocumento2 páginasLirik ThirdBilly Shan LastKagerooboroAinda não há avaliações
- ToxoplasmosisDocumento7 páginasToxoplasmosispamepomeAinda não há avaliações
- DMPADocumento5 páginasDMPABilly Shan LastKagerooboroAinda não há avaliações
- FIGO Clasificación HUA 2011Documento11 páginasFIGO Clasificación HUA 2011dickenskevinAinda não há avaliações
- Clin Infect Dis. 2008 Goldstein 554 66Documento13 páginasClin Infect Dis. 2008 Goldstein 554 66Billy Shan LastKagerooboroAinda não há avaliações
- Lyric Star-The Idolm@Ster Cinderella Project OP Season 1Documento2 páginasLyric Star-The Idolm@Ster Cinderella Project OP Season 1Billy Shan LastKagerooboroAinda não há avaliações
- Bab 6 Orako ProblemsDocumento4 páginasBab 6 Orako ProblemsBilly Shan LastKagerooboroAinda não há avaliações
- Vbac Risk Scoring AssessmentDocumento1 páginaVbac Risk Scoring AssessmentMaulana AdamAinda não há avaliações
- Vasomotor RhinitisDocumento6 páginasVasomotor RhinitisdewawsAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Transcranial DopplerDocumento3 páginasTranscranial DopplerAhmad NazirinAinda não há avaliações
- Veterinary Neurologic Rehabilitation The Rationale For ADocumento9 páginasVeterinary Neurologic Rehabilitation The Rationale For ACarolina Vargas VélezAinda não há avaliações
- Stroke - Practical Management 3rd EdDocumento998 páginasStroke - Practical Management 3rd Edprasad616100% (11)
- Presentation, Analysis and Interpretation of DataDocumento45 páginasPresentation, Analysis and Interpretation of DataJude EdubaAinda não há avaliações
- Albert Pinto Ko Tension Kyon Aaya? - A Risk Management CaseDocumento6 páginasAlbert Pinto Ko Tension Kyon Aaya? - A Risk Management Caseanweshacc100% (1)
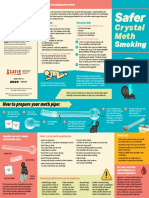
- CATIE SaferSmoking CrystalMeth E 2020 FINAL WEBDocumento2 páginasCATIE SaferSmoking CrystalMeth E 2020 FINAL WEBJeff PuglisiAinda não há avaliações
- EFNS Congress Vienna Semax AbstractDocumento60 páginasEFNS Congress Vienna Semax AbstractnontjeAinda não há avaliações
- Anticoagulation Oral Guideline 09 PDFDocumento21 páginasAnticoagulation Oral Guideline 09 PDFFhilla KanjaAinda não há avaliações
- Thesis Protocol: Suba Arul Devi (Post Graduate Student, Department of RadiodiagnosisDocumento21 páginasThesis Protocol: Suba Arul Devi (Post Graduate Student, Department of RadiodiagnosisJagan MaxAinda não há avaliações
- Coup de ChaleurDocumento16 páginasCoup de ChaleurEric CharpentierAinda não há avaliações
- Cryptogenic Stroke and Patent Foramen Ovale: Review Topic of The WeekDocumento8 páginasCryptogenic Stroke and Patent Foramen Ovale: Review Topic of The WeekferrevAinda não há avaliações
- CVA Case PresentationDocumento8 páginasCVA Case Presentationrichie_chan_2100% (3)
- Transient Ischemic AttacksDocumento10 páginasTransient Ischemic AttacksfabianounifenasAinda não há avaliações
- Nurses Need to Know About Stroke CareDocumento68 páginasNurses Need to Know About Stroke CareSuci Aning TAinda não há avaliações
- Panel 1: Aims of This Policy ViewDocumento10 páginasPanel 1: Aims of This Policy ViewSeptime TyasAinda não há avaliações
- Association of Serum Uric Acid Level with Coronary Artery DiseaseDocumento25 páginasAssociation of Serum Uric Acid Level with Coronary Artery Diseasedr.jkAinda não há avaliações
- Nursing Care Plan (NCP) : Date and Time Nursing Diagnosis Short - Term and Long - Term OutcomesDocumento2 páginasNursing Care Plan (NCP) : Date and Time Nursing Diagnosis Short - Term and Long - Term OutcomesDeanne Carla DalilisAinda não há avaliações
- English Aphasia United Best Practices Recommendations1Documento4 páginasEnglish Aphasia United Best Practices Recommendations1Tatiana Lopes FreitasAinda não há avaliações
- Manajemen StrokeDocumento253 páginasManajemen StrokeHappy Pramanda100% (2)
- Age at Menopause and Risk of Ischemic and Hemorrhagic StrokeDocumento9 páginasAge at Menopause and Risk of Ischemic and Hemorrhagic StrokeindanazulfaaAinda não há avaliações
- Day 3 Principles of Rehabilitation in Elderly The NewestDocumento43 páginasDay 3 Principles of Rehabilitation in Elderly The NewestaniendyawijayaAinda não há avaliações
- Diet 4 Stroke PreventionDocumento7 páginasDiet 4 Stroke PreventionNila AuthoriaAinda não há avaliações
- Brilinta (Ticagrelor) Tablets, For Oral UseDocumento2 páginasBrilinta (Ticagrelor) Tablets, For Oral UsePonpimol Odee BongkeawAinda não há avaliações
- College of Nursing: Pharmacological ManagementDocumento2 páginasCollege of Nursing: Pharmacological ManagementJOHN PEARL FERNANDEZAinda não há avaliações
- Apicon 2013 ScheduleDocumento51 páginasApicon 2013 Schedulesas7328Ainda não há avaliações
- Incidence of Aphasia in Ischemic StrokeDocumento9 páginasIncidence of Aphasia in Ischemic StrokeIndia SunshineAinda não há avaliações
- Haemophilia 1Documento10 páginasHaemophilia 1mahadirrosAinda não há avaliações
- Crisis of Hypertension Revised 1Documento57 páginasCrisis of Hypertension Revised 1keenmunir100% (4)
- ApraxiaDocumento15 páginasApraxiaMUHAMMAD BILALAinda não há avaliações
- 2020 AFIB 2020 - For WebDocumento166 páginas2020 AFIB 2020 - For WebHussein TfAinda não há avaliações