Você também pode gostar
- Business 7 JLangDocumento27 páginasBusiness 7 JLangpavaroti37Ainda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- European Consensus Conference On Faecal Microbiota Transplantation in Clinical PracticeDocumento13 páginasEuropean Consensus Conference On Faecal Microbiota Transplantation in Clinical Practicepavaroti3780% (56)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Blastocystis: To Treat or Not To Treat.: InvitedarticleDocumento6 páginasBlastocystis: To Treat or Not To Treat.: Invitedarticlepavaroti37Ainda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Euthrox CharacteristicsDocumento10 páginasEuthrox Characteristicspavaroti37Ainda não há avaliações
- Bacteriotherapy Faqs PDFDocumento17 páginasBacteriotherapy Faqs PDFpavaroti37100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- What Is Pep ?Documento11 páginasWhat Is Pep ?Dr vinod rainaAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Adam Abubakar Abdullahi TECHNICAL REPORTDocumento40 páginasAdam Abubakar Abdullahi TECHNICAL REPORTAdam AbubakarAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Case StudyDocumento12 páginasCase StudyEllen Diana CortelAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Biosafety and Bioethics of Biotechnology ABS-832: DR Attya Bhatti Assistant Professor Head of Department Asab-NustDocumento25 páginasBiosafety and Bioethics of Biotechnology ABS-832: DR Attya Bhatti Assistant Professor Head of Department Asab-NustVoltha HerryAinda não há avaliações
- KARM (Phycoviruses)Documento17 páginasKARM (Phycoviruses)KARM67% (3)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- CH 01 Lecture PresentationDocumento55 páginasCH 01 Lecture PresentationNguyen Ai LeAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Iej 04 2009Documento104 páginasIej 04 2009Israel CurveloAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Virus TableDocumento3 páginasVirus TableFrozenManAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Uv DoseDocumento6 páginasUv DoseRajesh DeshmukhAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- A Scientific Review About Green TeaDocumento11 páginasA Scientific Review About Green TeaMayra FlorAinda não há avaliações
- Covid-19 Epidemic EditorialDocumento2 páginasCovid-19 Epidemic EditorialAdam CayongcongAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- MicroPara 03 - Prokaryotic CellsDocumento23 páginasMicroPara 03 - Prokaryotic CellsJianne CaloAinda não há avaliações
- IcdDocumento180 páginasIcdFitri MoraAinda não há avaliações
- Yukgehnaish Etal PhageLeadsDocumento16 páginasYukgehnaish Etal PhageLeadsAugust ThomasenAinda não há avaliações
- A Brief Guide To Poultry Diseases ManagementDocumento29 páginasA Brief Guide To Poultry Diseases ManagementGrowel Agrovet Private Limited.83% (6)
- Mancuso 2018Documento19 páginasMancuso 2018Jessica Martinez CortezAinda não há avaliações
- LegionellaDocumento17 páginasLegionellaShubham Pareshkumar KadiwalaAinda não há avaliações
- Food Safety Case - The Fat Duck Norovirus Outbreak, UK - 2009Documento16 páginasFood Safety Case - The Fat Duck Norovirus Outbreak, UK - 2009OPGJrAinda não há avaliações
- Advanced Microbiology Course Plan: A Specific Plan For Teaching Microbiology in English To Non-Native SpeakersDocumento6 páginasAdvanced Microbiology Course Plan: A Specific Plan For Teaching Microbiology in English To Non-Native SpeakersMarco CruzAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The IMViC TestsDocumento4 páginasThe IMViC TestsVRampriyaAinda não há avaliações
- Acid Fast StainDocumento3 páginasAcid Fast StainGUIDO ERNESTO VILLOTA CALVACHIAinda não há avaliações
- Microbiology: OrthomyxovirusDocumento3 páginasMicrobiology: OrthomyxovirusJustin TayabanAinda não há avaliações
- IMMUNOLOGICAL AND BIOCHEMICAL RESPONSE FROM OLDER ADULTS WITH URINARY TRACT INFECTION TO UROPATHOGENIC Escherichia Coli VIRULENCE FACTORSDocumento5 páginasIMMUNOLOGICAL AND BIOCHEMICAL RESPONSE FROM OLDER ADULTS WITH URINARY TRACT INFECTION TO UROPATHOGENIC Escherichia Coli VIRULENCE FACTORSjavelezhAinda não há avaliações
- Lung AbscessDocumento7 páginasLung AbscessItha Maghfirah100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
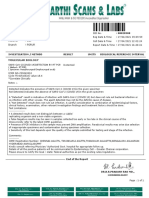
- Gopu.R:::: Patient Age / Sex 30 Y / Male BranchDocumento1 páginaGopu.R:::: Patient Age / Sex 30 Y / Male BranchGopu RAinda não há avaliações
- BioLumix NutraCBioLumix RMM Platform Featured in Latest Edition of NutraCos Journalos-Revise FINALDocumento3 páginasBioLumix NutraCBioLumix RMM Platform Featured in Latest Edition of NutraCos Journalos-Revise FINALAnnabel ElizabethAinda não há avaliações
- Aseptic Technique Lab ReportDocumento8 páginasAseptic Technique Lab ReportSleepyHead ˋωˊAinda não há avaliações
- Assignment Case Study BMS533Documento14 páginasAssignment Case Study BMS533Ahmad Nur AqmalAinda não há avaliações
- (23003235 - Bulletin of The Veterinary Institute in Pulawy) Microbiological Quality of Compound Feed Used in PolandDocumento6 páginas(23003235 - Bulletin of The Veterinary Institute in Pulawy) Microbiological Quality of Compound Feed Used in PolandfirewAinda não há avaliações
- HCCS BIOL 2320 Chapter 3 Lecture Notes 10eDocumento4 páginasHCCS BIOL 2320 Chapter 3 Lecture Notes 10ehoorAinda não há avaliações