Você também pode gostar
- Cranial Nerve Examination OSCE GuideDocumento26 páginasCranial Nerve Examination OSCE GuideAbdullah Basheer AL-AnaziAinda não há avaliações
- Notes - Notes - Ophthalmology PDFDocumento30 páginasNotes - Notes - Ophthalmology PDFRumana Ali100% (2)
- Performing Physical Assessment of The EyeDocumento14 páginasPerforming Physical Assessment of The Eyezyrine jhen100% (1)
- MCN Exam 2 Study Guide - CompleteDocumento87 páginasMCN Exam 2 Study Guide - CompleteColin MacKenzie100% (1)
- Neurologic Assessment Physiologic Changes With AgingDocumento4 páginasNeurologic Assessment Physiologic Changes With AgingDarl Dacdac100% (1)
- Otosclerosis and Menieres DiseaseDocumento5 páginasOtosclerosis and Menieres DiseaseYoko Mae YanoAinda não há avaliações
- 11 NCP Pressure UlcerDocumento6 páginas11 NCP Pressure UlcerICa MarlinaAinda não há avaliações
- SIM For Grade 3Documento21 páginasSIM For Grade 3Mark Cua96% (154)
- Uterine CancerDocumento20 páginasUterine Cancerzyrine jhen100% (4)
- Nursing Interview Guide To Collect Subjective Data From The Client Questions RationaleDocumento19 páginasNursing Interview Guide To Collect Subjective Data From The Client Questions RationaleKent Rebong100% (1)
- Schizophrenia PDFDocumento32 páginasSchizophrenia PDFJoyVee Pillagara-De LeonAinda não há avaliações
- Ophthalmology MCQsDocumento173 páginasOphthalmology MCQsvamshidh33% (3)
- GRP 20 Final Abscess Case StudyDocumento14 páginasGRP 20 Final Abscess Case StudyBorja, Kimberly GraceAinda não há avaliações
- CHAPTER 16 - Schizophrenia 2Documento15 páginasCHAPTER 16 - Schizophrenia 2RebeccaAinda não há avaliações
- NCPDocumento5 páginasNCPAthea Melosantos100% (1)
- Seizure PathophysiologyDocumento2 páginasSeizure PathophysiologyqwertyuiopAinda não há avaliações
- Medical BooksDocumento20 páginasMedical Booksapi-385347264% (14)
- The EyeDocumento48 páginasThe Eyezyrine jhen100% (1)
- EENT Disorders StudentsDocumento26 páginasEENT Disorders StudentsPye Antwan DelvaAinda não há avaliações
- The EyelidsDocumento64 páginasThe EyelidsSarahAinda não há avaliações
- Nursing Care Plan2Documento3 páginasNursing Care Plan2gaeLtorvzAinda não há avaliações
- PathophysiologyDocumento9 páginasPathophysiologySuzette PipoAinda não há avaliações
- MicrocephalyDocumento4 páginasMicrocephalykurei_bluflamedAinda não há avaliações
- MyelomeningoceleDocumento7 páginasMyelomeningocelemavefigAinda não há avaliações
- 51 100Documento18 páginas51 100Jaessa Feliciano100% (1)
- A Drug Study On FansidarDocumento7 páginasA Drug Study On FansidarCasey EmellanoAinda não há avaliações
- Nursing Informatics: Bachelor of Science in NursingDocumento4 páginasNursing Informatics: Bachelor of Science in NursingMichelle MallareAinda não há avaliações
- Alzheimeru2019s DiseaseDocumento17 páginasAlzheimeru2019s Diseaseapi-262538456100% (1)
- Cretenism Case StudyDocumento8 páginasCretenism Case StudyMonica Marie MoralesAinda não há avaliações
- ScriptDocumento2 páginasScriptKeith AquinoAinda não há avaliações
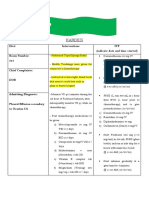
- Kardex: Diet: Interventions IVF (Indicate Date and Time Started) Room Number: 313Documento2 páginasKardex: Diet: Interventions IVF (Indicate Date and Time Started) Room Number: 313kuro hanabusaAinda não há avaliações
- GBS Nursing MangementDocumento21 páginasGBS Nursing MangementJoseph Namita SunnyAinda não há avaliações
- Annotated Group 2 Impetigo Concept Mapping 1Documento30 páginasAnnotated Group 2 Impetigo Concept Mapping 1DHANE ANN CAMPOSANOAinda não há avaliações
- Care For Patients With Alteration in Perception and CoordinationDocumento12 páginasCare For Patients With Alteration in Perception and Coordinationevlujtrep9690100% (1)
- Hiatal HerniaDocumento3 páginasHiatal HerniaJobelle AcenaAinda não há avaliações
- Concept Map Meningitis TheoryDocumento3 páginasConcept Map Meningitis TheoryMia AuliaAinda não há avaliações
- Septic Shock: Supervisor: DR Ali Haedar, Sp. EM FAHA Dinisa Novaurahmah Nanin Aprilia PutriDocumento42 páginasSeptic Shock: Supervisor: DR Ali Haedar, Sp. EM FAHA Dinisa Novaurahmah Nanin Aprilia PutriMutia Larasati AlbarAinda não há avaliações
- Chapter 35 Communication in Children - PilliteriDocumento20 páginasChapter 35 Communication in Children - PilliteriPhillip ChingAinda não há avaliações
- Brand NameDocumento5 páginasBrand NameJunrey AbarcaAinda não há avaliações
- Drug StudyDocumento15 páginasDrug StudyMarc AnchetaAinda não há avaliações
- Pathophysiology: Bipolar DisorderDocumento3 páginasPathophysiology: Bipolar DisorderPae EdejerAinda não há avaliações
- CATARACTS and GLAUCOMADocumento11 páginasCATARACTS and GLAUCOMAAmoroso, Marian Corneth D.Ainda não há avaliações
- Cap Grand Case PreDocumento46 páginasCap Grand Case PreMatty FelAinda não há avaliações
- Febrile SeizuresDocumento4 páginasFebrile Seizuresmgonzalez_29Ainda não há avaliações
- Iabetic Europathy: DR Saumya H Mittal Neurologist Sharda Hospital & Health CityDocumento39 páginasIabetic Europathy: DR Saumya H Mittal Neurologist Sharda Hospital & Health CityGhea SugihartiAinda não há avaliações
- Threatened Abortion ReportDocumento8 páginasThreatened Abortion ReportMohamad RaisAinda não há avaliações
- Pathophysiology HPN CvaDocumento1 páginaPathophysiology HPN Cvatresdos09Ainda não há avaliações
- NCP DisturbedDocumento2 páginasNCP DisturbedTrixie Anne GamotinAinda não há avaliações
- Cognitive Disorder QuizDocumento35 páginasCognitive Disorder QuizCamille Joy BaliliAinda não há avaliações
- Moira Mae B. Balite BSN 2A: Post Partum Care DefinitionDocumento5 páginasMoira Mae B. Balite BSN 2A: Post Partum Care DefinitionMoiraMaeBeridoBaliteAinda não há avaliações
- GRP 4 CLO 2 Concept Map PT 1 PDFDocumento14 páginasGRP 4 CLO 2 Concept Map PT 1 PDFMaria Lyn Ocariza ArandiaAinda não há avaliações
- Vitamin K (Phytomenadione) 2016: Indication Action Drug Type Trade Name Presentation Dosage / IntervalDocumento3 páginasVitamin K (Phytomenadione) 2016: Indication Action Drug Type Trade Name Presentation Dosage / IntervalDeni Yuda Adi SaputraAinda não há avaliações
- Definition of PneumoniaDocumento4 páginasDefinition of PneumoniaEmylia Ananda PutriAinda não há avaliações
- NCM117Documento20 páginasNCM117Marie Isabelle HerveraAinda não há avaliações
- Urinary System Disorders Practice Quiz #1 (50 Questions)Documento26 páginasUrinary System Disorders Practice Quiz #1 (50 Questions)Emy TandinganAinda não há avaliações
- NCP-Drug Study 2Documento4 páginasNCP-Drug Study 2hsiriaAinda não há avaliações
- Tetanus PathophysiologyDocumento7 páginasTetanus PathophysiologyWahyu Adhitya PrawirasatraAinda não há avaliações
- Ineffective Tissue Perfusion PDFDocumento4 páginasIneffective Tissue Perfusion PDFgcodouganAinda não há avaliações
- Counselling LetterDocumento1 páginaCounselling LetterSeann LorescoAinda não há avaliações
- 1retinal DetachmentDocumento5 páginas1retinal Detachmentsunny_jr_Ainda não há avaliações
- Nursing Care Plan For Subarachnoid HemorrhagicDocumento2 páginasNursing Care Plan For Subarachnoid HemorrhagicAshram Smart100% (1)
- Assisting: Venous Cut DownDocumento4 páginasAssisting: Venous Cut DownJimnah Rhodrick BontilaoAinda não há avaliações
- Nursing Care Plan: Ineffective CopingDocumento2 páginasNursing Care Plan: Ineffective CopingRosalinda SalvadorAinda não há avaliações
- Seizure DisorderDocumento4 páginasSeizure DisorderJohanna ChavezAinda não há avaliações
- Electrolyte Imbalance 1Documento3 páginasElectrolyte Imbalance 1Marius Clifford BilledoAinda não há avaliações
- Aging Perspective and Demography Ncm114 Gerontology Aging PerspectivesDocumento19 páginasAging Perspective and Demography Ncm114 Gerontology Aging PerspectivesLeslie CruzAinda não há avaliações
- CERTIFICATEDocumento2 páginasCERTIFICATEzyrine jhenAinda não há avaliações
- Cataract ExtractionDocumento4 páginasCataract Extractionselle726Ainda não há avaliações
- Visumax BrochureDocumento7 páginasVisumax Brochurekhairul ihsanAinda não há avaliações
- Eye NotesDocumento21 páginasEye NotesViswaAinda não há avaliações
- Igcse AccommodationDocumento3 páginasIgcse AccommodationChr1zFX4Ainda não há avaliações
- Sitasi JurnalDocumento2 páginasSitasi JurnalErfinaAinda não há avaliações
- Kevin Patrizio Final ResumeDocumento3 páginasKevin Patrizio Final Resumeapi-284037495Ainda não há avaliações
- Duane SyndromeDocumento27 páginasDuane SyndromeAlphamaleagainAinda não há avaliações
- Apo 201780Documento7 páginasApo 201780NNAinda não há avaliações
- Daftar Pustaka: Ed - III. Surabaya: Rumah Sakit Umum Dokter SoetomoDocumento2 páginasDaftar Pustaka: Ed - III. Surabaya: Rumah Sakit Umum Dokter Soetomomisbahul jannahAinda não há avaliações
- Cataract in Adults - UpToDateDocumento35 páginasCataract in Adults - UpToDateSantiago Martinez ValeroAinda não há avaliações
- Daftar PustakaDocumento2 páginasDaftar Pustakamelita Aditya SariAinda não há avaliações
- Rockaway Times 7617Documento44 páginasRockaway Times 7617Peter J. MahonAinda não há avaliações
- The Challenges of Ophthalmic-Residency Education in The PhilippinesDocumento11 páginasThe Challenges of Ophthalmic-Residency Education in The PhilippinesAjit ChambalAinda não há avaliações
- Logbook New 1Documento61 páginasLogbook New 1Shantanu SaxenaAinda não há avaliações
- Elective Course Topics-1Documento9 páginasElective Course Topics-1Rebecca WongAinda não há avaliações
- Jurnal AutorefractometerDocumento11 páginasJurnal AutorefractometerNeida Valeria DanunAinda não há avaliações
- Management of Eyelid DefectDocumento29 páginasManagement of Eyelid DefectMuhammad AbdillahAinda não há avaliações
- By Prapatsorn Patikulsila, MD.: Ophthalmology AbbreviationsDocumento4 páginasBy Prapatsorn Patikulsila, MD.: Ophthalmology AbbreviationsDoaa SaifAinda não há avaliações
- Lesson Plans - VisionDocumento5 páginasLesson Plans - VisionZach SanfordAinda não há avaliações
- Anatomy of The Image-Forming EyeDocumento23 páginasAnatomy of The Image-Forming EyekupukupuAinda não há avaliações
- Block M2 EYE Distribution by MMCDocumento3 páginasBlock M2 EYE Distribution by MMCF ParikhAinda não há avaliações
- Anatomi Dan Fisiologi KorneaDocumento133 páginasAnatomi Dan Fisiologi KorneaAriyanie NurtaniaAinda não há avaliações
- Refrat Dwinkha Mata RefraksiDocumento17 páginasRefrat Dwinkha Mata RefraksiDwinkha Agita PAinda não há avaliações
- ARMD M Optom 4 TH SemesterDocumento78 páginasARMD M Optom 4 TH Semestertanishqa eye careAinda não há avaliações
- Eye Pathology: Dr. Jusuf FantoniDocumento8 páginasEye Pathology: Dr. Jusuf Fantonitutor tujuhAinda não há avaliações