Você também pode gostar
- Diseases of the Liver and Biliary TreeNo EverandDiseases of the Liver and Biliary TreeAnnarosa FloreaniAinda não há avaliações
- Pathogenesis and Management of Hepatolithiasis: A Report of Two CasesDocumento3 páginasPathogenesis and Management of Hepatolithiasis: A Report of Two CasesBenny KurniawanAinda não há avaliações
- International Journal of Infectious Diseases: Anshuman Pandey, Shakeel Masood, Namrata P. AwasthiDocumento3 páginasInternational Journal of Infectious Diseases: Anshuman Pandey, Shakeel Masood, Namrata P. Awasthijohanna monsalveAinda não há avaliações
- 191 FullDocumento3 páginas191 FullPaediatrics CMC VelloreAinda não há avaliações
- Electronic Image of The Month: A Rare Tumor of The Common Hepatic Duct Causing Biliary ObstructionDocumento2 páginasElectronic Image of The Month: A Rare Tumor of The Common Hepatic Duct Causing Biliary ObstructionDeborah Anasthasia PakpahanAinda não há avaliações
- Absence of The Cystic Duct:: A Case Report, A Review of LiteratureDocumento3 páginasAbsence of The Cystic Duct:: A Case Report, A Review of LiteratureBolivar IseaAinda não há avaliações
- Case Report Hepato FinalDocumento29 páginasCase Report Hepato FinalBangkit PutrawanAinda não há avaliações
- Calcagno 2018Documento10 páginasCalcagno 2018cut normaya putriAinda não há avaliações
- 201 203 AbdominalDocumento3 páginas201 203 AbdominalManal Salah DorghammAinda não há avaliações
- JFP 1994 11 v39 I5 Giant Ovarian Cyst Mimicking AscitesDocumento3 páginasJFP 1994 11 v39 I5 Giant Ovarian Cyst Mimicking AscitesLuciana Da CruzAinda não há avaliações
- Case Series of Unusual Causes Intestinal Obstruction in Infants and ChildrenDocumento9 páginasCase Series of Unusual Causes Intestinal Obstruction in Infants and ChildrenSnega KaranAinda não há avaliações
- Carol I SyndromeDocumento3 páginasCarol I SyndromefebrymaharaniputriAinda não há avaliações
- Biliary AtresiaDocumento13 páginasBiliary AtresiaGündüz AğayevAinda não há avaliações
- "Inflammatory Pseudotumor" of Liver With Occlusive PhlebitisDocumento6 páginas"Inflammatory Pseudotumor" of Liver With Occlusive PhlebitisLizeth Paola TellezAinda não há avaliações
- Case Report: Streptococcus AnginosusDocumento4 páginasCase Report: Streptococcus AnginosusIesanu MaraAinda não há avaliações
- 19Documento3 páginas19Elizabeth ToapantaAinda não há avaliações
- Heterotopic Pancreas of The Gallbladder Associated With Chronic CholecystitisDocumento3 páginasHeterotopic Pancreas of The Gallbladder Associated With Chronic CholecystitisAziz EzoAinda não há avaliações
- Annsurg00231 0116Documento9 páginasAnnsurg00231 0116Dodo MnsiAinda não há avaliações
- Surgical Management of Carolis Disease i (2)Documento2 páginasSurgical Management of Carolis Disease i (2)suraj rajpurohitAinda não há avaliações
- An Unusual Cause of Acute Abdomend Gas-Forming Liver Abscess Due To Salmonella EnteritidisDocumento4 páginasAn Unusual Cause of Acute Abdomend Gas-Forming Liver Abscess Due To Salmonella EnteritidisMenda JangWooyoung SooyoungsterAinda não há avaliações
- Z - 2001-01 - Nonfunctioning Islet Cell Carcinoma of The Pancreas Associated With Massive Intra-Abdominal HemorrhageDocumento5 páginasZ - 2001-01 - Nonfunctioning Islet Cell Carcinoma of The Pancreas Associated With Massive Intra-Abdominal HemorrhageNawzad SulayvaniAinda não há avaliações
- Peritoneal Encapsulation: A Rare Cause of Small Bowel ObstructionDocumento3 páginasPeritoneal Encapsulation: A Rare Cause of Small Bowel ObstructionNatalindah Jokiem Woecandra T. D.Ainda não há avaliações
- Crigm2019 8907068Documento4 páginasCrigm2019 8907068AlixAinda não há avaliações
- Diagnosis and Management of Hepatolithiasis in An.242Documento4 páginasDiagnosis and Management of Hepatolithiasis in An.242Mike ChristantiAinda não há avaliações
- Chronic Empyaema Gall BladderDocumento2 páginasChronic Empyaema Gall BladderSuresh Kalyanasundar (Professor)Ainda não há avaliações
- Colo-uterineFistulaaRareComplicationofDiverticularDiseasDocumento8 páginasColo-uterineFistulaaRareComplicationofDiverticularDiseasRandy SaputraAinda não há avaliações
- At Two: Was SeDocumento3 páginasAt Two: Was Seida ayu agung WijayantiAinda não há avaliações
- Renal Tuberculosis Mimicking Renal Cell CarcinomaDocumento3 páginasRenal Tuberculosis Mimicking Renal Cell CarcinomaNingsih 09Ainda não há avaliações
- Incidentally Exploration of The Fusiform Cystic Duct 2024 International JourDocumento4 páginasIncidentally Exploration of The Fusiform Cystic Duct 2024 International JourRonald QuezadaAinda não há avaliações
- Pneumatosis Cystoides Intestinalis: Report of Two Cases: M. Turan, M. S En, R. EgılmezDocumento3 páginasPneumatosis Cystoides Intestinalis: Report of Two Cases: M. Turan, M. S En, R. EgılmezzixdiddyAinda não há avaliações
- Use Only: Investigating A Rare Cause of Intestinal OcclusionDocumento2 páginasUse Only: Investigating A Rare Cause of Intestinal OcclusionDannyMichelleAinda não há avaliações
- Triple GallbladerDocumento12 páginasTriple GallbladerRudy Arindra WijayaAinda não há avaliações
- Dafpus LiverDocumento2 páginasDafpus LiverMenda JangWooyoung SooyoungsterAinda não há avaliações
- Bile Duct Perforation in Children: Is It Truly Spontaneous?: Case ReportDocumento4 páginasBile Duct Perforation in Children: Is It Truly Spontaneous?: Case ReportMuhammad Bin NasserAinda não há avaliações
- Bile Leak CaseDocumento6 páginasBile Leak CaseDimas ErlanggaAinda não há avaliações
- 1999-07 - Intraductal Papillary-Mucinous Tumor of The Pancreas - Presentation in A Young Adult PDFDocumento4 páginas1999-07 - Intraductal Papillary-Mucinous Tumor of The Pancreas - Presentation in A Young Adult PDFNawzad SulayvaniAinda não há avaliações
- Insignis Surgery 2 Gallbladder and Extrahepatic Biliary SystemDocumento7 páginasInsignis Surgery 2 Gallbladder and Extrahepatic Biliary SystemPARADISE JanoAinda não há avaliações
- Lamp IranDocumento5 páginasLamp IranTanwilyAinda não há avaliações
- Laparoscopy and Primary Diffuse MalignantDocumento5 páginasLaparoscopy and Primary Diffuse Malignantmalvina.sekolonik911Ainda não há avaliações
- Ce (Ra1) F (Ac) Pf1 (Agak) Pfa (Ak) PB (NC Ag) PN (SL)Documento3 páginasCe (Ra1) F (Ac) Pf1 (Agak) Pfa (Ak) PB (NC Ag) PN (SL)Anwesa ChakrabortyAinda não há avaliações
- Spontaneous Rupture of Pyonephrosis Leading To PyoperitoneumDocumento3 páginasSpontaneous Rupture of Pyonephrosis Leading To PyoperitoneumsamiAinda não há avaliações
- S2116 Novel Presentation of Rectal Granular Cell.2116Documento2 páginasS2116 Novel Presentation of Rectal Granular Cell.2116dianisaindiraAinda não há avaliações
- Pancreatic Adenocarcinoma Mimicking PseudocystDocumento3 páginasPancreatic Adenocarcinoma Mimicking PseudocystInternational Journal of Innovative Science and Research TechnologyAinda não há avaliações
- HydronephrosisDocumento3 páginasHydronephrosisCarla AlmerolAinda não há avaliações
- Small Bowel Obstruction Due To Phytobezoars: Report of Four Cases and Literature ReviewDocumento5 páginasSmall Bowel Obstruction Due To Phytobezoars: Report of Four Cases and Literature ReviewAna Laura Sánchez BaltazarAinda não há avaliações
- PIIS0016508515000359Documento2 páginasPIIS0016508515000359Christofel JomanAinda não há avaliações
- Post LapChole Bile LeaksDocumento41 páginasPost LapChole Bile LeaksIfeanyichukwu OgbonnayaAinda não há avaliações
- emerg-3-168Documento2 páginasemerg-3-168Randy SaputraAinda não há avaliações
- Stomach volvulus case reportDocumento7 páginasStomach volvulus case reportChristabella Natalia WijayaAinda não há avaliações
- Infectious Diseases: Extra-Pulmonary Infection: A CaseDocumento5 páginasInfectious Diseases: Extra-Pulmonary Infection: A CaseAyush JainAinda não há avaliações
- Hepatocellular Carcinoma Causing Severe.1057Documento1 páginaHepatocellular Carcinoma Causing Severe.1057Vardan KocharAinda não há avaliações
- Jurnal Literatur Case Series 1Documento4 páginasJurnal Literatur Case Series 1Debby LadadoAinda não há avaliações
- Unusual Presentation of Choriocarcinoma: Case ReportDocumento2 páginasUnusual Presentation of Choriocarcinoma: Case ReportcuyAinda não há avaliações
- Pyloric BandDocumento6 páginasPyloric BandRia RfAinda não há avaliações
- EN Acute Pancreatitis As A Complication ofDocumento5 páginasEN Acute Pancreatitis As A Complication ofShandy JonnerAinda não há avaliações
- 3 CamplobacterDocumento3 páginas3 CamplobacterUlmoTolkienAinda não há avaliações
- Chylous Ascites 3Documento3 páginasChylous Ascites 3Nur atikaAinda não há avaliações
- In-Depth Review: Nonocclusive Mesenteric Ischemia: A Lethal Complication in Peritoneal Dialysis PatientsDocumento6 páginasIn-Depth Review: Nonocclusive Mesenteric Ischemia: A Lethal Complication in Peritoneal Dialysis PatientsFernandoAinda não há avaliações
- Duplication of Gallbladder: Case ReportDocumento3 páginasDuplication of Gallbladder: Case ReportVenanda RianAinda não há avaliações
- Bazo Errante 2016 REVISED Ijtra1601084Documento4 páginasBazo Errante 2016 REVISED Ijtra1601084luisalfredo_montesAinda não há avaliações
- 2020 - Detecting Ethambutol Resistance in Mycobacterium Tuberculosis Isolates in China A Comparison Between Phenotypic Drug Susceptibility Testing Methods and DNA Sequencing of embABDocumento7 páginas2020 - Detecting Ethambutol Resistance in Mycobacterium Tuberculosis Isolates in China A Comparison Between Phenotypic Drug Susceptibility Testing Methods and DNA Sequencing of embABNurul RifqianiAinda não há avaliações
- Pathophysiology and Treatment of Neuropathic Pain AssociatedDocumento9 páginasPathophysiology and Treatment of Neuropathic Pain AssociatedNurul RifqianiAinda não há avaliações
- Bus Navi 2Documento1 páginaBus Navi 2Nurul RifqianiAinda não há avaliações
- Bus Navi 1Documento1 páginaBus Navi 1Nurul RifqianiAinda não há avaliações
- Review Article: Cholangiocarcinoma: Biology, Clinical Management, and Pharmacological PerspectivesDocumento14 páginasReview Article: Cholangiocarcinoma: Biology, Clinical Management, and Pharmacological PerspectivesNurul RifqianiAinda não há avaliações
- Sy Ringo My EliaDocumento13 páginasSy Ringo My EliaNurul RifqianiAinda não há avaliações
- Worsening or Development of Syringomyelia FollowingDocumento6 páginasWorsening or Development of Syringomyelia FollowingNurul RifqianiAinda não há avaliações
- Ni Hms 407962Documento26 páginasNi Hms 407962Nurul RifqianiAinda não há avaliações
- A Review of The Clinical Diagnosis and Therapy of Cholangiocarcinoma PDFDocumento14 páginasA Review of The Clinical Diagnosis and Therapy of Cholangiocarcinoma PDFNurul RifqianiAinda não há avaliações
- A Review of The Clinical Diagnosis and Therapy of CholangiocarcinomaDocumento14 páginasA Review of The Clinical Diagnosis and Therapy of CholangiocarcinomaNurul RifqianiAinda não há avaliações
- Cholangiocarcinoma Current Knowledge and New DevelopmentsDocumento14 páginasCholangiocarcinoma Current Knowledge and New DevelopmentsNurul RifqianiAinda não há avaliações
- Recent Update in The Management of Invasive Fungal InfectionDocumento30 páginasRecent Update in The Management of Invasive Fungal Infectionanoop61100% (2)
- Romeo Seeks Poison from ApothecaryDocumento5 páginasRomeo Seeks Poison from ApothecaryMichelle FranciscoAinda não há avaliações
- 4Documento13 páginas4Juan Carlos Hernandez CriadoAinda não há avaliações
- Language Leader Pre-Int Unit 4Documento7 páginasLanguage Leader Pre-Int Unit 4SimayAinda não há avaliações
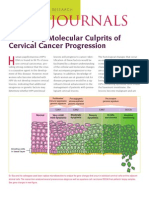
- CC Mol CulpritsDocumento3 páginasCC Mol Culpritsirfan_2ansariAinda não há avaliações
- Maternal and Newborn Nursing AbbreviationsDocumento3 páginasMaternal and Newborn Nursing AbbreviationsjamesAinda não há avaliações
- Đề Thi Giữa Kì Trúng Tủ - Mục Tiêu 9+Documento5 páginasĐề Thi Giữa Kì Trúng Tủ - Mục Tiêu 9+OriAinda não há avaliações
- Summative TestDocumento3 páginasSummative TestBaby Sharl100% (13)
- Endocrine Drugs: Pituitary, Thyroid, Parathyroid, and Adrenal DisordersDocumento29 páginasEndocrine Drugs: Pituitary, Thyroid, Parathyroid, and Adrenal DisordersPam LalaAinda não há avaliações
- Municipality of Buenavista, Bohol, Philippines - A Situational Analysis, IncompleteDocumento25 páginasMunicipality of Buenavista, Bohol, Philippines - A Situational Analysis, IncompleteMark Johnuel Duavis0% (1)
- SANITIZING TUNNEL PPT FinalDocumento12 páginasSANITIZING TUNNEL PPT FinalSOUMYA HAinda não há avaliações
- Review of "The Hot Zone-The Terrifying True Story of The Origins of The Ebola Virus"Documento7 páginasReview of "The Hot Zone-The Terrifying True Story of The Origins of The Ebola Virus"David EishenAinda não há avaliações
- Pglo PowerpointDocumento24 páginasPglo Powerpointapi-358036976100% (1)
- PoliomyelitisDocumento4 páginasPoliomyelitisapi-3710926100% (2)
- Florygene Kris A. Disagon HypervolemiaDocumento4 páginasFlorygene Kris A. Disagon HypervolemiaFlorygene Kris DisagonAinda não há avaliações
- Rubella & FlavivirusDocumento53 páginasRubella & Flaviviruskiedd_04Ainda não há avaliações
- Research ADocumento61 páginasResearch APrincess GarduceAinda não há avaliações
- ResearchDocumento75 páginasResearchKabeer Golechha100% (1)
- Soal SoalDocumento3 páginasSoal SoalAdiguna DarmantoAinda não há avaliações
- Activity 8-Applying Descriptive Analytics: A Year of Data Insights in The Time of COVID-19Documento3 páginasActivity 8-Applying Descriptive Analytics: A Year of Data Insights in The Time of COVID-19Louie Jay LayderosAinda não há avaliações
- Salmonella Infections Clinical Immunological and Molecular Aspects Advances in Molecular and Cellular Microbiology PDFDocumento402 páginasSalmonella Infections Clinical Immunological and Molecular Aspects Advances in Molecular and Cellular Microbiology PDFFredAinda não há avaliações
- Parasite Profile ChartDocumento40 páginasParasite Profile Chartapi-324380555100% (3)
- Vocabulary 11Documento3 páginasVocabulary 11Mirko Flores JimenezAinda não há avaliações
- The Use of Antibiotics in Surgical PatientsDocumento58 páginasThe Use of Antibiotics in Surgical PatientsajcheeAinda não há avaliações
- 01 - Introduction To DentistryDocumento18 páginas01 - Introduction To Dentistrymichal ben meronAinda não há avaliações
- Ch.1-16 Answers CombinedDocumento144 páginasCh.1-16 Answers Combinedbrandon culpepper100% (11)
- Bacte PPT #10 - Gram Negative Bacilli Part 1Documento52 páginasBacte PPT #10 - Gram Negative Bacilli Part 1Marl EstradaAinda não há avaliações
- SACMC - 19052020 - Slides For MoHmediabriefingDocumento21 páginasSACMC - 19052020 - Slides For MoHmediabriefingBranko Brkic93% (15)
- Tubulointerstitial Diseases: Dr. Raid JastaniaDocumento48 páginasTubulointerstitial Diseases: Dr. Raid JastaniaThomas McconnellAinda não há avaliações
- Project-Sterilization of Water Using Bleaching PowderDocumento17 páginasProject-Sterilization of Water Using Bleaching PowderKamaljoshi40% (2)