Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Contemporary Nursing 8th Cherry Test BankDocumento9 páginasContemporary Nursing 8th Cherry Test BankSaifoqqAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- APA Citations For Nursing TextbooksDocumento1 páginaAPA Citations For Nursing Textbooksbbianca199075% (4)
- Pathophysiology of Neonatal Sepsis Secondary To Neonatal PneumoniaDocumento4 páginasPathophysiology of Neonatal Sepsis Secondary To Neonatal Pneumoniapaul andrew laranjo asuncion80% (5)
- Globocan 2020Documento2 páginasGlobocan 2020Dicky keyAinda não há avaliações
- Elc590 Informative Speech About InsomniaDocumento5 páginasElc590 Informative Speech About InsomniaANGJELLY ALLYA NGAUHAinda não há avaliações
- Hirschsprung NCM 109 Case PresentationDocumento10 páginasHirschsprung NCM 109 Case PresentationValerie LeddaAinda não há avaliações
- Evidence-Based Practice in Pediatric Physical Therapy by BarryDocumento14 páginasEvidence-Based Practice in Pediatric Physical Therapy by BarryFe TusAinda não há avaliações
- The Diagram Shows How A Company Called HB Office RDocumento1 páginaThe Diagram Shows How A Company Called HB Office RbugakAinda não há avaliações
- ACOG - External Cephalic Version PDFDocumento10 páginasACOG - External Cephalic Version PDFPat CabanitAinda não há avaliações
- Addressing The Gaps in Nutritional Care Before and During PregnancyDocumento12 páginasAddressing The Gaps in Nutritional Care Before and During PregnancyBushra KainaatAinda não há avaliações
- Prospectus: 1 ReservationsDocumento8 páginasProspectus: 1 ReservationsvarunAinda não há avaliações
- Schizophrenia This OneDocumento44 páginasSchizophrenia This OneAnabelle RicoAinda não há avaliações
- Pappas Bikhazi 2023 Babe Ruth S Anaplastic Epidermoid Carcinoma of The NasopharynxDocumento5 páginasPappas Bikhazi 2023 Babe Ruth S Anaplastic Epidermoid Carcinoma of The NasopharynxVinoster ProductionAinda não há avaliações
- Back Pain During PregnancyDocumento3 páginasBack Pain During PregnancyDr. Sadhana KalaAinda não há avaliações
- Disability MatrixDocumento21 páginasDisability MatrixAngelika MendozaAinda não há avaliações
- The Influence of Music in Horror Games (Final Draft)Documento7 páginasThe Influence of Music in Horror Games (Final Draft)Panther LenoXAinda não há avaliações
- Effects of Sprint Interval Training and Body.24Documento8 páginasEffects of Sprint Interval Training and Body.24Maxwell MartinsAinda não há avaliações
- Food SafetyDocumento2 páginasFood SafetymacmanueAinda não há avaliações
- Quadruple Aim in HealthcareDocumento2 páginasQuadruple Aim in HealthcareMarimiel PagulayanAinda não há avaliações
- Aravind Eye Care Systems: Providing Total Eye Care To The Rural PopulationDocumento13 páginasAravind Eye Care Systems: Providing Total Eye Care To The Rural PopulationAvik BorahAinda não há avaliações
- Laparoscopic Appendectomy SurgeryDocumento2 páginasLaparoscopic Appendectomy SurgeryNycoAinda não há avaliações
- Fatal Airway Obstruction Due To Ludwig'sDocumento6 páginasFatal Airway Obstruction Due To Ludwig'sRegina MugopalAinda não há avaliações
- Synthesis PaperDocumento7 páginasSynthesis Paperapi-379148533Ainda não há avaliações
- Lecture 1 Health, Safety & Environment (HSE)Documento23 páginasLecture 1 Health, Safety & Environment (HSE)A to z type videosAinda não há avaliações
- Overcoming Obesogenic Environments: A Qualitative Study Exploring Mechanisms of Healthy EatersDocumento10 páginasOvercoming Obesogenic Environments: A Qualitative Study Exploring Mechanisms of Healthy EatersCristina Saldias PorrasAinda não há avaliações
- Pres 2 PastpapersDocumento190 páginasPres 2 PastpapersOdetteAinda não há avaliações
- Handbook: Master of Social Work StudiesDocumento26 páginasHandbook: Master of Social Work StudiesSukhman ChahalAinda não há avaliações
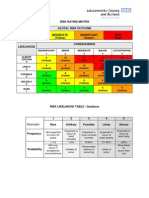
- Example of A NHS Risk Rating MatrixDocumento2 páginasExample of A NHS Risk Rating MatrixRochady SetiantoAinda não há avaliações
- Sq20-030 - Fact Sheet - Informed Consent - Nsqhs-8.9aDocumento4 páginasSq20-030 - Fact Sheet - Informed Consent - Nsqhs-8.9aPedro Medeiros JrAinda não há avaliações
- State of The World's Midwifery 2014: A Universal Pathway - A Woman's Right To HealthDocumento228 páginasState of The World's Midwifery 2014: A Universal Pathway - A Woman's Right To HealthUNFPA SoWMYAinda não há avaliações