Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- 6th Central Pay Commission Salary CalculatorDocumento15 páginas6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Aim Healthy WeightDocumento44 páginasAim Healthy WeightJuan Herrera SalazarAinda não há avaliações
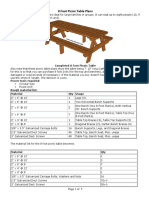
- 8 Foot Picnic Table Plans: Build a Large Seating Picnic TableDocumento5 páginas8 Foot Picnic Table Plans: Build a Large Seating Picnic Tabletom2susanAinda não há avaliações
- SUMMER SALADS AND SANDWICHESDocumento4 páginasSUMMER SALADS AND SANDWICHEStom2susanAinda não há avaliações
- The History and Future of KAATSU TrainingDocumento5 páginasThe History and Future of KAATSU TrainingRosaneLacerdaAinda não há avaliações
- Cwu O&g 1 PPROMDocumento13 páginasCwu O&g 1 PPROMFaris Mohd Nasir100% (1)
- AnyView A8 A6 A5 A3 Patient Monitor User Manual-2011E2Documento276 páginasAnyView A8 A6 A5 A3 Patient Monitor User Manual-2011E2Medipro78% (9)
- Scheduling Procedures Cath LabDocumento3 páginasScheduling Procedures Cath Labrajneeshchd100% (1)
- Dialysis in Older PatientsDocumento220 páginasDialysis in Older PatientsMiguel Angel Molinero100% (1)
- Arduino For Ham Radio PresentationDocumento50 páginasArduino For Ham Radio Presentationtom2susan100% (2)
- Pathophysiology of Arrhythmias: Causes and MechanismsDocumento53 páginasPathophysiology of Arrhythmias: Causes and MechanismsAmanuel MaruAinda não há avaliações
- Where To Get Help For Selective MutismDocumento2 páginasWhere To Get Help For Selective MutismTee Kok KeongAinda não há avaliações
- Doh Requirements Level 1 HospitalDocumento50 páginasDoh Requirements Level 1 HospitalFerdinand M. Turbanos100% (4)
- Supraspinatus TendinitisDocumento23 páginasSupraspinatus TendinitisTafzz Sailo0% (1)
- CKD PathophysiologyDocumento1 páginaCKD Pathophysiologylloyd_santino67% (3)
- San Pedro Hospital of Davao City, Inc.: Nurses' NotesDocumento2 páginasSan Pedro Hospital of Davao City, Inc.: Nurses' NotesSophia Jay LaurieAinda não há avaliações
- Instrucciones de Uso VamosDocumento94 páginasInstrucciones de Uso VamosfjvillamunozAinda não há avaliações
- Enron: The Good, The Bad, The LessonsDocumento20 páginasEnron: The Good, The Bad, The Lessonstom2susanAinda não há avaliações
- 3 Day Patrol Duty Roster PDFDocumento1 página3 Day Patrol Duty Roster PDFtom2susanAinda não há avaliações
- White House Guidelines For Reopening EconomyDocumento18 páginasWhite House Guidelines For Reopening EconomyJeffrey DunetzAinda não há avaliações
- Iss Utilization 2017b-TaggedDocumento112 páginasIss Utilization 2017b-TaggedMohammedKhalifaAinda não há avaliações
- ISS Packet Operation On 70cm-20161113Documento1 páginaISS Packet Operation On 70cm-20161113tom2susanAinda não há avaliações
- Chokes and Shot PatternDocumento5 páginasChokes and Shot Patterntom2susanAinda não há avaliações
- The Kit Carson TrailDocumento4 páginasThe Kit Carson Trailtom2susanAinda não há avaliações
- Bennett Spring Hatch Chart Fly Fishing GuideDocumento1 páginaBennett Spring Hatch Chart Fly Fishing Guidetom2susanAinda não há avaliações
- Bandanas Carryout MenuDocumento3 páginasBandanas Carryout Menutom2susanAinda não há avaliações
- VA Form 21-2680 Exam for Housebound or Aid and Attendance BenefitsDocumento2 páginasVA Form 21-2680 Exam for Housebound or Aid and Attendance Benefitstom2susanAinda não há avaliações
- BabbosDocumento2 páginasBabbostom2susanAinda não há avaliações
- Crushed Red ColumbiaDocumento2 páginasCrushed Red Columbiatom2susanAinda não há avaliações
- Cloud ChartDocumento2 páginasCloud Charttom2susanAinda não há avaliações
- Pad Aha:Acc 2005 Exec SummaryDocumento75 páginasPad Aha:Acc 2005 Exec Summarytom2susanAinda não há avaliações
- Thyroid Nodules TI-RADSDocumento1 páginaThyroid Nodules TI-RADStom2susanAinda não há avaliações
- Federal Explosives Law and Regulations 2012 Atf-P-5400-7 PDFDocumento112 páginasFederal Explosives Law and Regulations 2012 Atf-P-5400-7 PDFtom2susanAinda não há avaliações
- Therapeutic Shoes For Persons With Diabetes PresentationDocumento67 páginasTherapeutic Shoes For Persons With Diabetes Presentationtom2susanAinda não há avaliações
- Blue CardDocumento1 páginaBlue Cardtom2susanAinda não há avaliações
- ABI CodingDocumento2 páginasABI Codingtom2susanAinda não há avaliações
- Antenna AccessoriesDocumento5 páginasAntenna Accessoriestom2susanAinda não há avaliações
- ABI Measuring ACP Chart PDFDocumento1 páginaABI Measuring ACP Chart PDFtom2susanAinda não há avaliações
- Digital ModesDocumento34 páginasDigital Modestom2susanAinda não há avaliações
- Choosing An AntennaDocumento7 páginasChoosing An AntennaJunjun BedrijoAinda não há avaliações
- HF Amplifiers Versus Antennas-One Ham's OpinionDocumento5 páginasHF Amplifiers Versus Antennas-One Ham's OpinionvirginiaAinda não há avaliações
- Borgstein ENTbookDocumento191 páginasBorgstein ENTbookdokhenAinda não há avaliações
- Dental and Craniomaxillofacial Implant SurgeryDocumento35 páginasDental and Craniomaxillofacial Implant SurgeryJean Carlos Barbosa FerreiraAinda não há avaliações
- Andre Hannah NursingresumeDocumento1 páginaAndre Hannah Nursingresumeapi-450112281Ainda não há avaliações
- Reading Comprehension-II: Max. Marks: 24 No. of Qs. 24 Time: 20 Min. Date: ......... /........ /...............Documento3 páginasReading Comprehension-II: Max. Marks: 24 No. of Qs. 24 Time: 20 Min. Date: ......... /........ /...............Hitesh MishraAinda não há avaliações
- Elizabeth Resume 2Documento3 páginasElizabeth Resume 2api-252417118Ainda não há avaliações
- A Clinical Decision Support Framework ForDocumento5 páginasA Clinical Decision Support Framework FordineshshaAinda não há avaliações
- Venous DiseaseDocumento45 páginasVenous DiseaseNinch Nagac100% (1)
- A Placebo-Controlled Test of Cognitive-Behavioral Therapy For Comorbid Insomnia in Older AdultsDocumento11 páginasA Placebo-Controlled Test of Cognitive-Behavioral Therapy For Comorbid Insomnia in Older Adultssilvia dwi puspitaAinda não há avaliações
- Thesis T3003 PDFDocumento99 páginasThesis T3003 PDFNor HidayahAinda não há avaliações
- Bpac Inr Poem 2006 WVDocumento26 páginasBpac Inr Poem 2006 WVmrezasyahliAinda não há avaliações
- Lesson 1.A: First Aid for Common Outdoor EmergenciesDocumento30 páginasLesson 1.A: First Aid for Common Outdoor EmergenciesAnonymous LToOBqDAinda não há avaliações
- CASENGHI, Buruli Ulcer FINAL - WatermarkedDocumento1 páginaCASENGHI, Buruli Ulcer FINAL - WatermarkedjackstewartbriggsAinda não há avaliações
- The Effectiveness of Pre-Operative Deep BreathingDocumento5 páginasThe Effectiveness of Pre-Operative Deep BreathingJulenda CintarinovaAinda não há avaliações
- Nursing Care PlanDocumento4 páginasNursing Care PlanJoshua Pascasio100% (1)
- Dall Miles Surgical ProtocolDocumento16 páginasDall Miles Surgical Protocolfarnaz_2647334Ainda não há avaliações
- 2012 FDA Warning Letter - MedtronicDocumento7 páginas2012 FDA Warning Letter - MedtronicWhatYou HaventSeenAinda não há avaliações
- Principles of Pharmacokinetics and PharmacodynamicsDocumento136 páginasPrinciples of Pharmacokinetics and PharmacodynamicsDidiAinda não há avaliações
- Debate ScriptDocumento5 páginasDebate ScriptzahraumaiyaAinda não há avaliações