Você também pode gostar
- Intra-Abdominal HypertensionDocumento3 páginasIntra-Abdominal HypertensionClark SavageAinda não há avaliações
- Abdominal Compartment SyndromeDocumento22 páginasAbdominal Compartment SyndromeHalbana Al MaududyAinda não há avaliações
- G3 IAH and ACSDocumento29 páginasG3 IAH and ACSRoshin Mae E. TejeroAinda não há avaliações
- Intra-Abdominal Hypertension: Andrew William L. AquinoDocumento15 páginasIntra-Abdominal Hypertension: Andrew William L. AquinoEdelrose LapitanAinda não há avaliações
- FUNDAMENTALSAnswer and RationaleDocumento20 páginasFUNDAMENTALSAnswer and RationaleRandyAinda não há avaliações
- Group 5 - Hemodialysis - Chronic Kidney FailureDocumento31 páginasGroup 5 - Hemodialysis - Chronic Kidney FailureKimberly Abella CabreraAinda não há avaliações
- Aplastic AnemiaDocumento11 páginasAplastic AnemiaToni Shiraishi-Aque RuizAinda não há avaliações
- Understanding Traumatic Brain InjuryDocumento43 páginasUnderstanding Traumatic Brain InjurySilvanaPutriAinda não há avaliações
- Hepatic Encephalopathy and ComaDocumento19 páginasHepatic Encephalopathy and ComaJas Castro JoveroAinda não há avaliações
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsNo EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsAinda não há avaliações
- NCM100 Cystoclysis CareDocumento2 páginasNCM100 Cystoclysis CarecchiechieAinda não há avaliações
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNo EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideAinda não há avaliações
- 780 Adult Cardio Resp Assess DSTDocumento10 páginas780 Adult Cardio Resp Assess DSTGursangeet Kaur100% (1)
- 422 Shock EssayDocumento6 páginas422 Shock Essayapi-364149810Ainda não há avaliações
- Pediatric Cardio-Respiratory AssessmentDocumento9 páginasPediatric Cardio-Respiratory AssessmentRicky SpideyAinda não há avaliações
- Management of Chest TubeDocumento22 páginasManagement of Chest TubeFatima Hafza SahiddinAinda não há avaliações
- Principles of Sterile TechniqueDocumento2 páginasPrinciples of Sterile TechniqueAliah M. AngodAinda não há avaliações
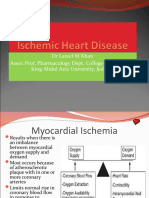
- Ischemic Heart Disease Revised LMKDocumento50 páginasIschemic Heart Disease Revised LMKLateef KhanAinda não há avaliações
- Care of The Clients With Problems in Acute Biologic Crisis: Ateneo de Zamboanga UniversityDocumento3 páginasCare of The Clients With Problems in Acute Biologic Crisis: Ateneo de Zamboanga UniversityGrant Wynn ArnucoAinda não há avaliações
- GROUP 2 Evidence Based Practice Nursing ManagementDocumento68 páginasGROUP 2 Evidence Based Practice Nursing ManagementIlert Kliene Tantoy ArcayaAinda não há avaliações
- NURSING EMERGENCIES. 10 BASED TEST QUESTIONS WITH BIBLIOGRAPHYNo EverandNURSING EMERGENCIES. 10 BASED TEST QUESTIONS WITH BIBLIOGRAPHYAinda não há avaliações
- The Battle Against Covid-19 Filipino American Healthcare Workers on the Frontlines of the Pandemic ResponseNo EverandThe Battle Against Covid-19 Filipino American Healthcare Workers on the Frontlines of the Pandemic ResponseAinda não há avaliações
- Fluid ElectrolyteDocumento115 páginasFluid ElectrolytePaul EbenezerAinda não há avaliações
- A. Cardiac Failure: Biologic CrisisDocumento11 páginasA. Cardiac Failure: Biologic CrisisJillian CaumbanAinda não há avaliações
- Cellular AberrationDocumento71 páginasCellular AberrationMichael CoronadoAinda não há avaliações
- Fluid Balance in Clinical PracticeDocumento8 páginasFluid Balance in Clinical Practicefernando_vaz2010100% (1)
- Blood AdministrationDocumento35 páginasBlood AdministrationnurminieAinda não há avaliações
- Fluid and ElectrolytesDocumento29 páginasFluid and ElectrolytesLinh Tra100% (1)
- Intro-ESRD Case StudyDocumento2 páginasIntro-ESRD Case StudyAngel SamonteAinda não há avaliações
- Case Study: Congestive Heart FailureDocumento7 páginasCase Study: Congestive Heart FailureXI-E / 21 / MARY TRIANAAinda não há avaliações
- Acute Biologic Crisis 1Documento45 páginasAcute Biologic Crisis 1Nina OaipAinda não há avaliações
- Medical Surgical Nursing 4 BulletsDocumento5 páginasMedical Surgical Nursing 4 BulletsQueen ElizabethAinda não há avaliações
- 1 Fluid Volume Excess Chronic Renal Failure Nursing Care PlansDocumento3 páginas1 Fluid Volume Excess Chronic Renal Failure Nursing Care PlansMichael Baylon DueñasAinda não há avaliações
- Lesson 2 NCM 103Documento3 páginasLesson 2 NCM 103KIM KALIBAYAinda não há avaliações
- Hemodialysis FinalDocumento40 páginasHemodialysis Finalrose FolwersAinda não há avaliações
- Sinus Rhythms: Dysrhythmia Recognition & ManagementDocumento29 páginasSinus Rhythms: Dysrhythmia Recognition & Managementkamel6Ainda não há avaliações
- What Is Hypertensive NephropathyDocumento11 páginasWhat Is Hypertensive NephropathyIvy Pamanian DeldaAinda não há avaliações
- Emergency Management of DKADocumento12 páginasEmergency Management of DKAtinzioAinda não há avaliações
- GI Diagnostic TestsDocumento7 páginasGI Diagnostic TestspatzieAinda não há avaliações
- Journal in Medical WardDocumento4 páginasJournal in Medical WardApol PenAinda não há avaliações
- Urinary Tract Infections in ChildrenDocumento56 páginasUrinary Tract Infections in ChildrenmedpedshospitalistAinda não há avaliações
- Copd Power PointDocumento33 páginasCopd Power PointRINIAinda não há avaliações
- Fluid and Electrolyte NotesDocumento6 páginasFluid and Electrolyte NotesAshley H Locklear100% (1)
- GROUP 3 - CASE STUDY - TraumaDocumento5 páginasGROUP 3 - CASE STUDY - TraumaDinarkram Rabreca EculAinda não há avaliações
- TriageDocumento8 páginasTriageSarah GuintoAinda não há avaliações
- 8. Care of Child With GI Dysfunction (1) ءءءءDocumento44 páginas8. Care of Child With GI Dysfunction (1) ءءءءNuhaAinda não há avaliações
- Cardiac TestsDocumento17 páginasCardiac TestsGiorgiana pAinda não há avaliações
- Med-Surge QuestionsDocumento17 páginasMed-Surge QuestionsRosa0% (1)
- Central Venous PressureDocumento10 páginasCentral Venous PressureAngelo ArquizaAinda não há avaliações
- Bipolar Brochure English FINAL 150109 PDFDocumento9 páginasBipolar Brochure English FINAL 150109 PDFIka M. HendrajayaAinda não há avaliações
- Hepatic Encephalopathy: Causes, Tests, and Treatment OptionsNo EverandHepatic Encephalopathy: Causes, Tests, and Treatment OptionsNota: 3.5 de 5 estrelas3.5/5 (2)
- Hepatobiliary Disorders: Katrina Saludar Jimenez, R. NDocumento42 páginasHepatobiliary Disorders: Katrina Saludar Jimenez, R. NKatrinaJimenezAinda não há avaliações
- PHARMACOLOGY - Midterms 1.6-Fluid and Electrolyte TRANSDocumento13 páginasPHARMACOLOGY - Midterms 1.6-Fluid and Electrolyte TRANSNooneAinda não há avaliações
- Thrombolytics, Anticoags, Antiplatelets PDFDocumento21 páginasThrombolytics, Anticoags, Antiplatelets PDFrachelkdoAinda não há avaliações
- Acne: Etiopathogenesis and Its Management: Usha Kataria, Dinesh ChhillarDocumento7 páginasAcne: Etiopathogenesis and Its Management: Usha Kataria, Dinesh ChhillarBayu Surya DanaAinda não há avaliações
- Nihms 1063023Documento38 páginasNihms 1063023Bayu Surya DanaAinda não há avaliações
- Di Kota Pekalongan Dwi Edi Wibowo, Saeful Marom: Dwiediwibowo73@yahoo - Co.idDocumento11 páginasDi Kota Pekalongan Dwi Edi Wibowo, Saeful Marom: Dwiediwibowo73@yahoo - Co.idBayu Surya DanaAinda não há avaliações
- Acute Tonsillitis On The Pediatric District: Etiologic Diagnosis and TreatmentDocumento7 páginasAcute Tonsillitis On The Pediatric District: Etiologic Diagnosis and TreatmentBayu Surya DanaAinda não há avaliações
- Pediatric Appendicitis Clinical Presentation - History, Physical ExaminationDocumento5 páginasPediatric Appendicitis Clinical Presentation - History, Physical ExaminationBayu Surya DanaAinda não há avaliações
- Nonalcoholic Fatty Liver Disease A Systematic ReviewDocumento11 páginasNonalcoholic Fatty Liver Disease A Systematic ReviewBayu Surya DanaAinda não há avaliações
- Tonsillitis and Peritonsillar Abscess Workup - Approach Considerations, Lab Studies, Imaging StudiesDocumento2 páginasTonsillitis and Peritonsillar Abscess Workup - Approach Considerations, Lab Studies, Imaging StudiesBayu Surya DanaAinda não há avaliações
- Clinical Presentation and Epidemiology of Stroke - A Study of 100 CasesDocumento4 páginasClinical Presentation and Epidemiology of Stroke - A Study of 100 CasesBayu Surya DanaAinda não há avaliações
- Prevalence of Fusobacterium Necrophorum in Tonsils From Patients With Chronic TonsillitisDocumento6 páginasPrevalence of Fusobacterium Necrophorum in Tonsils From Patients With Chronic TonsillitisBayu Surya DanaAinda não há avaliações
- Chronic Kidney Disease Clinical Presentation - History, Physical ExaminationDocumento2 páginasChronic Kidney Disease Clinical Presentation - History, Physical ExaminationBayu Surya DanaAinda não há avaliações
- Causes and Clinical Characteristics of Headache in Ischaemic StrokeDocumento3 páginasCauses and Clinical Characteristics of Headache in Ischaemic StrokeBayu Surya DanaAinda não há avaliações
- 2009 Article 9236Documento5 páginas2009 Article 9236Bayu Surya DanaAinda não há avaliações
- Pap Smear - Overview, Indications, PreparationDocumento11 páginasPap Smear - Overview, Indications, PreparationBayu Surya DanaAinda não há avaliações
- Human Papillomavirus and HPV Vaccines: A ReviewDocumento8 páginasHuman Papillomavirus and HPV Vaccines: A ReviewBayu Surya DanaAinda não há avaliações
- Doi 10.4297/najms.2010.2468Documento7 páginasDoi 10.4297/najms.2010.2468Bayu Surya DanaAinda não há avaliações
- Over The Counter Wart Removal ProductsDocumento2 páginasOver The Counter Wart Removal ProductsAlex DA CostaAinda não há avaliações
- Breast Care in BreastfeedingDocumento11 páginasBreast Care in BreastfeedingBella Cy LopezAinda não há avaliações
- Thursday September 29Documento9 páginasThursday September 29Ken HoiAinda não há avaliações
- Meningitis - 2018Documento55 páginasMeningitis - 2018Abraham Anaely100% (1)
- Jurnal KesehatanDocumento17 páginasJurnal KesehatanDiani Rista SariAinda não há avaliações
- NATIONAL INSURANCE - National Parivar Mediclaim PolicyDocumento31 páginasNATIONAL INSURANCE - National Parivar Mediclaim PolicyStigan IndiaAinda não há avaliações
- Failure To Thrive With NotesDocumento45 páginasFailure To Thrive With NotesJason Jimmy Lee PillayAinda não há avaliações
- s1299 Can Alpha Feto Protein Level Be Used As A.1299Documento2 páginass1299 Can Alpha Feto Protein Level Be Used As A.1299Chia Diamante NegroAinda não há avaliações
- March 2013 Board of Nursing NoticesDocumento528 páginasMarch 2013 Board of Nursing NoticesJames LindonAinda não há avaliações
- In Memoriam Allan Cott, M.D. 1910-1993: Journal of Orthomolecular Medicine. He WasDocumento4 páginasIn Memoriam Allan Cott, M.D. 1910-1993: Journal of Orthomolecular Medicine. He WasSchwab RealHumanAinda não há avaliações
- Closed Door - NP1 (SC)Documento7 páginasClosed Door - NP1 (SC)13rokenAinda não há avaliações
- Diseases of The Spleen Burnett PDFDocumento146 páginasDiseases of The Spleen Burnett PDFDrAbhay Meghaji ChhedaAinda não há avaliações
- Petition To Save St. Lawrence Psych CenterDocumento256 páginasPetition To Save St. Lawrence Psych Centerpritchie10Ainda não há avaliações
- (CPG) Philippine Guidelines On Periodic Health Examination: Screening For Neoplastic DiseasesDocumento194 páginas(CPG) Philippine Guidelines On Periodic Health Examination: Screening For Neoplastic DiseasesBianca Watanabe - RatillaAinda não há avaliações
- Haematolgy MDT WebDocumento2 páginasHaematolgy MDT WebbfdboiiAinda não há avaliações
- End of LifeDocumento31 páginasEnd of LifeSimran JosanAinda não há avaliações
- QuestionnaireDocumento10 páginasQuestionnaireLyrad MagpantayAinda não há avaliações
- Nabh ChecklistDocumento2 páginasNabh ChecklistJatoveda Haldar100% (1)
- أساسيات التمريض نظرى (1) (1) 2222Documento8 páginasأساسيات التمريض نظرى (1) (1) 2222Pŕìncëş Ğï ŘlAinda não há avaliações
- Example On Infection Control - Failure Modes and Effects Analysis Tool Process Data ReportDocumento2 páginasExample On Infection Control - Failure Modes and Effects Analysis Tool Process Data ReportEskadmas BelayAinda não há avaliações
- Kolkata HospitalDocumento24 páginasKolkata HospitalKoushikKc ChatterjeeAinda não há avaliações
- Eatern Equatoria State PresentationDocumento24 páginasEatern Equatoria State PresentationMayom MabuongAinda não há avaliações
- Final Revise ThesisDocumento33 páginasFinal Revise ThesisKeplot Lirpa91% (11)
- FILE 20221001 131945 FILE 20220506 115242 APSIC-CSSD-COE-Program-2022Documento7 páginasFILE 20221001 131945 FILE 20220506 115242 APSIC-CSSD-COE-Program-2022dvhoangAinda não há avaliações
- New Trends in The Diagnosis and Management of HypertensionDocumento10 páginasNew Trends in The Diagnosis and Management of HypertensionJULIANA SANCHEZAinda não há avaliações
- Sarcoptes Scabiei (Infection With)Documento4 páginasSarcoptes Scabiei (Infection With)Dinna KarlinaAinda não há avaliações
- NCP Risk For InfectionDocumento3 páginasNCP Risk For InfectionuzumakiharuAinda não há avaliações
- A Case of Patient AI, Who Came in Due To Sore ThroatDocumento16 páginasA Case of Patient AI, Who Came in Due To Sore ThroatLovelle LopezAinda não há avaliações
- Educational Visits Consent Form GreenwichDocumento2 páginasEducational Visits Consent Form Greenwichmiskinmusic123Ainda não há avaliações
- Pathophysiology of IBDDocumento11 páginasPathophysiology of IBDOktarina Heni SunandarAinda não há avaliações