Você também pode gostar
- Proposed Grad Plan Stacy BrunsgaardDocumento1 páginaProposed Grad Plan Stacy Brunsgaardapi-477606437Ainda não há avaliações
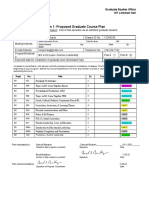
- Form 1: Proposed Graduate Course Plan: Bussmanbr@mnstate - EduDocumento2 páginasForm 1: Proposed Graduate Course Plan: Bussmanbr@mnstate - Eduapi-426106794Ainda não há avaliações
- Webber Plan of StudyDocumento1 páginaWebber Plan of Studyapi-555909235Ainda não há avaliações
- Form 1Documento2 páginasForm 1api-244827434Ainda não há avaliações
- GIA FormDocumento12 páginasGIA FormCatherine CacayuranAinda não há avaliações
- IRS-Proposal Form-1Documento5 páginasIRS-Proposal Form-1sameer.khanAinda não há avaliações
- Cihak Plan of Study 2Documento1 páginaCihak Plan of Study 2api-556229871Ainda não há avaliações
- Division Order/ Memorandum/Advisory: Division of City of San FernandoDocumento9 páginasDivision Order/ Memorandum/Advisory: Division of City of San FernandogiansulakisosuAinda não há avaliações
- Wiscad Portfolio Plan Due June 30 ADocumento3 páginasWiscad Portfolio Plan Due June 30 Aapi-344737206Ainda não há avaliações
- Griffin MDocumento2 páginasGriffin Mapi-533966514Ainda não há avaliações
- PGP Final Eval Form 2017Documento2 páginasPGP Final Eval Form 2017api-232727324Ainda não há avaliações
- Program of StudyDocumento2 páginasProgram of Studyapi-307568494Ainda não há avaliações
- Itpdp ExampleDocumento2 páginasItpdp Exampleapi-244827434Ainda não há avaliações
- Ganfield ResumeDocumento3 páginasGanfield Resumeapi-663025888Ainda não há avaliações
- Revised ReserchThesis-MS-Pre-Req-08Feb2018Documento4 páginasRevised ReserchThesis-MS-Pre-Req-08Feb2018matiqAinda não há avaliações
- ActionPlan Sample 12 15 2015Documento4 páginasActionPlan Sample 12 15 2015joel ruizAinda não há avaliações
- Looking ForwardDocumento6 páginasLooking Forwardapi-455761336Ainda não há avaliações
- F-1 Curricular Practical Training Application: Family FirstDocumento4 páginasF-1 Curricular Practical Training Application: Family FirstSrinivasan TAinda não há avaliações
- 11660Documento1 página11660Fahima KhanAinda não há avaliações
- A Look ForwardDocumento6 páginasA Look Forwardapi-421128974Ainda não há avaliações
- Memo Mea 2022 Guidelines 1Documento11 páginasMemo Mea 2022 Guidelines 1JAHYRAH BARTOLOMEAinda não há avaliações
- Sample: School Action PlanDocumento4 páginasSample: School Action PlanBinibini BeeAinda não há avaliações
- IRS ProposalForm MS ProjectMgt 18 0123Documento5 páginasIRS ProposalForm MS ProjectMgt 18 0123sameer.khanAinda não há avaliações
- K - 5 Prep Academy R. Samana September 2013Documento6 páginasK - 5 Prep Academy R. Samana September 2013Barney StinsonAinda não há avaliações
- Broderius Program of Study 2Documento2 páginasBroderius Program of Study 2api-556451334Ainda não há avaliações
- Individualised Education Plan: This Is A Working Document To Be ReviewedDocumento7 páginasIndividualised Education Plan: This Is A Working Document To Be Reviewedapi-285147634Ainda não há avaliações
- Program of StudyDocumento1 páginaProgram of Studyapi-515950929Ainda não há avaliações
- Administrative & Supervisory PlanDocumento5 páginasAdministrative & Supervisory PlanJherivil Defrenjeal Canonigo AlferezAinda não há avaliações
- 2017-2018 IdpDocumento7 páginas2017-2018 Idpapi-373664036Ainda não há avaliações
- Permit To Study 1Documento7 páginasPermit To Study 1Cla RaAinda não há avaliações
- RSM 7204 Integration and Analysis (Capstone) Course SyllabusDocumento8 páginasRSM 7204 Integration and Analysis (Capstone) Course SyllabusAman DattaAinda não há avaliações
- Master's degree plan for educational managementDocumento1 páginaMaster's degree plan for educational managementSalmaAinda não há avaliações
- Student Government Awards On Elem. and High SchoolDocumento14 páginasStudent Government Awards On Elem. and High SchoolAdrian CatapatAinda não há avaliações
- 2017-04-06 Spring 2017 GAISEDocumento1 página2017-04-06 Spring 2017 GAISEShakeel Ahmad KhanAinda não há avaliações
- Johnson Bryan 2017-18 Appraisal 6.21.18-FinalDocumento15 páginasJohnson Bryan 2017-18 Appraisal 6.21.18-FinalDan LehrAinda não há avaliações
- Teacher Education Department: Field Study ProgramDocumento3 páginasTeacher Education Department: Field Study ProgramCherry BenitezAinda não há avaliações
- Circular - Selection of Prefects For The Academic Year 2024 - 25Documento3 páginasCircular - Selection of Prefects For The Academic Year 2024 - 25vihaanpnaik2024Ainda não há avaliações
- Resume CfisdDocumento1 páginaResume Cfisdapi-498711832Ainda não há avaliações
- DepEd SOCCSKSARGEN Redeploys Teachers to Address ShortagesDocumento8 páginasDepEd SOCCSKSARGEN Redeploys Teachers to Address ShortagesEric John VegafriaAinda não há avaliações
- Bergren Plan of StudyDocumento1 páginaBergren Plan of Studyapi-570074789Ainda não há avaliações
- Reference: Deped Memorandum (No. 165, S. 2017) To Be Indicated in The Perpetual Index Under The Following SubjectsDocumento3 páginasReference: Deped Memorandum (No. 165, S. 2017) To Be Indicated in The Perpetual Index Under The Following SubjectsRam KuizonAinda não há avaliações
- Career Readiness Development in Middle and High SchoolDocumento53 páginasCareer Readiness Development in Middle and High SchoolAbdulmalikAinda não há avaliações
- 2016-2017 IdpDocumento7 páginas2016-2017 Idpapi-373664036Ainda não há avaliações
- Assignment For PG Diploma in Information Security - PGDIS - Jan - 2020 PDFDocumento12 páginasAssignment For PG Diploma in Information Security - PGDIS - Jan - 2020 PDFVijayendran PAinda não há avaliações
- Crownfield Infant and Nursery SchoolDocumento7 páginasCrownfield Infant and Nursery SchoolLucy EFAinda não há avaliações
- DepEd Order Gradution RitesDocumento2 páginasDepEd Order Gradution RitesRudolph Amiel A. DaganzoAinda não há avaliações
- Project Monitoring Tool for RaW 2 ProgramDocumento2 páginasProject Monitoring Tool for RaW 2 ProgramNino IgnacioAinda não há avaliações
- Bilingual Effect FinalDocumento34 páginasBilingual Effect FinalKinza MalikAinda não há avaliações
- Pa Log 4Documento1 páginaPa Log 4api-610107403Ainda não há avaliações
- Department of Education: Schools Division Office of Camarines SurDocumento3 páginasDepartment of Education: Schools Division Office of Camarines SurMC MirandaAinda não há avaliações
- School Improvement PlanDocumento6 páginasSchool Improvement PlanJayson ArmodiaAinda não há avaliações
- SLAC1Documento2 páginasSLAC1JESSICA ARNADOAinda não há avaliações
- Schmitz Program of Study Signed 1 1Documento1 páginaSchmitz Program of Study Signed 1 1api-556441910Ainda não há avaliações
- Claire e Raykovitz ResumeDocumento1 páginaClaire e Raykovitz Resumeapi-519293566Ainda não há avaliações
- Szabi ST: Proposal Form Independent Research Study (Computer Sciences) Semester - 20Documento4 páginasSzabi ST: Proposal Form Independent Research Study (Computer Sciences) Semester - 20Abbas NaqviAinda não há avaliações
- SIP Design TemplateDocumento16 páginasSIP Design TemplateMary Joy TorratoAinda não há avaliações
- Department of Education: Learning and Development (L&D) ProposalDocumento4 páginasDepartment of Education: Learning and Development (L&D) ProposalPEDRITO DULAYAinda não há avaliações
- Greenwood High College & Career CounsellingDocumento14 páginasGreenwood High College & Career CounsellingAlinaAinda não há avaliações
- Mark Motherway Educator LicenseDocumento1 páginaMark Motherway Educator Licenseapi-338364690Ainda não há avaliações
- MsumacademicrecordDocumento1 páginaMsumacademicrecordapi-338364690Ainda não há avaliações
- J StefanpracticumcontractcompletionDocumento1 páginaJ Stefanpracticumcontractcompletionapi-338364690Ainda não há avaliações
- Reflectiveessay pdf1Documento10 páginasReflectiveessay pdf1api-338364690Ainda não há avaliações
- Msum Practicum GuideDocumento97 páginasMsum Practicum Guideapi-338364690Ainda não há avaliações
- MarkmotherwayacademicrecordDocumento4 páginasMarkmotherwayacademicrecordapi-338364690Ainda não há avaliações
- Mark JresumeDocumento2 páginasMark Jresumeapi-338364690Ainda não há avaliações
- J Stefan Contract Approval FormDocumento1 páginaJ Stefan Contract Approval Formapi-338364690Ainda não há avaliações
- J StefanfieldsupervisorformDocumento1 páginaJ Stefanfieldsupervisorformapi-338364690Ainda não há avaliações
- J AkrepracticumcontractcompletionDocumento1 páginaJ Akrepracticumcontractcompletionapi-338364690Ainda não há avaliações
- 2017-18 Student HandbookDocumento43 páginas2017-18 Student Handbookapi-338364690Ainda não há avaliações
- Student Contract FormDocumento1 páginaStudent Contract Formapi-338364690Ainda não há avaliações
- 2017-18 Teacher HandbookDocumento27 páginas2017-18 Teacher Handbookapi-338364690Ainda não há avaliações
- Chapter 10 MCQs: External Growth FactorsDocumento3 páginasChapter 10 MCQs: External Growth Factorsprince ahenkoraAinda não há avaliações
- HDR 2000 enDocumento309 páginasHDR 2000 enJM Manicap-OtomanAinda não há avaliações
- Volterravito PDFDocumento6 páginasVolterravito PDFTracey MorinAinda não há avaliações
- Trifles DiscussionDocumento11 páginasTrifles Discussionapi-242602081Ainda não há avaliações
- Mas Que Nada LessonDocumento2 páginasMas Que Nada Lessondl1485Ainda não há avaliações
- Lesson Plan in Science Grade 6Documento4 páginasLesson Plan in Science Grade 6Myreen Certeza100% (3)
- Kinder 1Documento2 páginasKinder 1api-266484104Ainda não há avaliações
- "HIV/AIDS Policy in South Korea," Cho Byoung-HeeDocumento3 páginas"HIV/AIDS Policy in South Korea," Cho Byoung-HeekhulawAinda não há avaliações
- Students Cumulative RecordDocumento2 páginasStudents Cumulative RecordJanaiah Ruth PateAinda não há avaliações
- Local Case StudyDocumento6 páginasLocal Case StudyMonica LisingAinda não há avaliações
- Business Plan Project: A Step-by-Step Guide To Writing A Business PlanDocumento13 páginasBusiness Plan Project: A Step-by-Step Guide To Writing A Business PlanBusiness Expert Press80% (79)
- 1793 Smollan Brochure All InteractiveDocumento240 páginas1793 Smollan Brochure All InteractiveAnonymous pz6teEr100% (1)
- Personal Development PlanDocumento12 páginasPersonal Development PlanHasan Mahmood100% (1)
- The One Room School - Williamsport's LegacyDocumento120 páginasThe One Room School - Williamsport's LegacyNancyAinda não há avaliações
- International Cme On Surgical Pathology 2013Documento12 páginasInternational Cme On Surgical Pathology 2013Nataraj ThambiAinda não há avaliações
- English HWDocumento11 páginasEnglish HWAyushAinda não há avaliações
- Effect of Reciprocal Teaching and Motivation On Reading Comprehension2016Documento5 páginasEffect of Reciprocal Teaching and Motivation On Reading Comprehension2016Aqila HafeezAinda não há avaliações
- 2014 Book TheCatalyzingMind PDFDocumento307 páginas2014 Book TheCatalyzingMind PDFCatalina Henríquez100% (1)
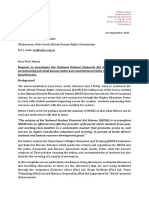
- SAHRC Complaint Against NSFAS 2023 - SignedDocumento4 páginasSAHRC Complaint Against NSFAS 2023 - SignedSune Payne- Daily MaverickAinda não há avaliações
- Howto - Writing Task 1 GeneralDocumento29 páginasHowto - Writing Task 1 GeneralellenlionAinda não há avaliações
- Developing Good Study HabitsDocumento18 páginasDeveloping Good Study HabitsN-jay Ivan Daclitan Sicat100% (1)
- Transcription of TED TalksDocumento6 páginasTranscription of TED TalksJamela Jade T. BonostroAinda não há avaliações
- Linguaskill Test Format: The Reading and Listening Module Is Adaptive, So There Is Not A Fixed Number of Questions. EachDocumento2 páginasLinguaskill Test Format: The Reading and Listening Module Is Adaptive, So There Is Not A Fixed Number of Questions. EachJosé ManuelAinda não há avaliações
- TS EAMCET Detailed NotificationDocumento4 páginasTS EAMCET Detailed NotificationNishit kumar100% (1)
- LM-0354 Gramatica Inglesa III PresenDocumento6 páginasLM-0354 Gramatica Inglesa III PresenLuis MongeAinda não há avaliações
- Essential Visual Design Goals and PrinciplesDocumento7 páginasEssential Visual Design Goals and PrinciplesMiftahul JannahAinda não há avaliações
- Teaching Strategies to Improve English Learners' SkillsDocumento8 páginasTeaching Strategies to Improve English Learners' SkillsFerdauzea AyadaAinda não há avaliações
- Sciebooks A Web Based SelfDocumento17 páginasSciebooks A Web Based SelfJell Vicor OpenaAinda não há avaliações
- Convention On The Elimination of All Forms of Discrimination Against Women (Cedaw)Documento3 páginasConvention On The Elimination of All Forms of Discrimination Against Women (Cedaw)JubsAinda não há avaliações
- Entrepreneurship: Entrepreneurial Mind SetDocumento24 páginasEntrepreneurship: Entrepreneurial Mind SetFaizan AhmadAinda não há avaliações