Você também pode gostar
- Prácticas de anatomía con enfoque odontológicoNo EverandPrácticas de anatomía con enfoque odontológicoAinda não há avaliações
- Fibras de SharpeyDocumento217 páginasFibras de Sharpeysanabria_161250% (2)
- Diseñar Los Patrones de AparatologiaDocumento19 páginasDiseñar Los Patrones de AparatologiaPeter RootsAinda não há avaliações
- Presentacion de Tesis de TaniaDocumento55 páginasPresentacion de Tesis de Taniacesarpaulo4100% (2)
- Clase 2 Exodoncia y CirugiaDocumento22 páginasClase 2 Exodoncia y CirugiaMilena AndrićAinda não há avaliações
- Mantenedores de EspacioDocumento8 páginasMantenedores de EspacioLeonardo CruzAinda não há avaliações
- Tesis Documento FinalDocumento123 páginasTesis Documento FinalLiceth Herrera MartinezAinda não há avaliações
- FibrotomíaDocumento8 páginasFibrotomíaLiliAinda não há avaliações
- Presentacion Funcion PulparDocumento21 páginasPresentacion Funcion PulparalisespinozaAinda não há avaliações
- Exposicion Cirugia Dientes IncluidosDocumento10 páginasExposicion Cirugia Dientes Incluidosアランザとビクター 愛しているAinda não há avaliações
- Apunte ResinasDocumento12 páginasApunte ResinasMacarena Cortes MAinda não há avaliações
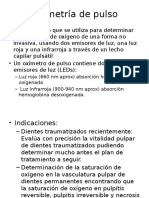
- Oximetría de PulsoDocumento6 páginasOximetría de PulsoHernandez Luis SamAinda não há avaliações
- Bioquimica Oral - SalivaDocumento13 páginasBioquimica Oral - SalivaCristian Pincheira Araya100% (1)
- Mascara Facial PDFDocumento19 páginasMascara Facial PDFJaimeMeza100% (1)
- Hábitos Bucales DeformantesDocumento16 páginasHábitos Bucales DeformantesElizabeth De StefanoAinda não há avaliações
- Instrumental Odp 2013 PDFDocumento3 páginasInstrumental Odp 2013 PDFAna Beatriz Mardones VarelaAinda não há avaliações
- INFORME 1 Principios Basicos de La OrtodonciaDocumento12 páginasINFORME 1 Principios Basicos de La OrtodonciaNoemi EscobarAinda não há avaliações
- DTM IDocumento29 páginasDTM ICindyBernalMAinda não há avaliações
- Paladar Duro EnaoDocumento40 páginasPaladar Duro EnaoGermanLoopezzAinda não há avaliações
- Adhesión DentalDocumento23 páginasAdhesión DentalRAQUEL ALDAMA UAEHAinda não há avaliações
- Forma de ArcadasDocumento6 páginasForma de ArcadasVivi MejiaAinda não há avaliações
- Sobredentadura (Clase) PDFDocumento7 páginasSobredentadura (Clase) PDFAlina Venete100% (1)
- Examen OrtoDocumento4 páginasExamen OrtoKuno Ferdyel100% (1)
- Técnicas de Apertura Cameral en Molares - WordDocumento2 páginasTécnicas de Apertura Cameral en Molares - WordYanira Zavaleta CastilloAinda não há avaliações
- Tecnicas de Anestesia MaxilarDocumento81 páginasTecnicas de Anestesia MaxilarBRISA ANETTE SOLIS GUZMANAinda não há avaliações
- CLASIFICACIÓN DR LISCHER PreguntasDocumento4 páginasCLASIFICACIÓN DR LISCHER PreguntasGloria HdzSchzAinda não há avaliações
- Desarrollo y Erupción DentariaDocumento18 páginasDesarrollo y Erupción Dentariaesedisambul100% (1)
- Retenedores Indirectos RESUMENDocumento3 páginasRetenedores Indirectos RESUMENEstefanía PuelloAinda não há avaliações
- Manejo Del Paciente Diabético en El Consultorio OdontológicoDocumento20 páginasManejo Del Paciente Diabético en El Consultorio OdontológicoOdontología 1/1Ainda não há avaliações
- AislamientoDocumento51 páginasAislamientoAdrian VenturaAinda não há avaliações
- Tumores Odontógenos MixtosDocumento4 páginasTumores Odontógenos MixtosYessie Yance D AraneaAinda não há avaliações
- Formacion Del Hueso en NinosDocumento5 páginasFormacion Del Hueso en Ninosanon_571797493Ainda não há avaliações
- Bioseguridad en OdontologiaDocumento12 páginasBioseguridad en Odontologiapaolo mendezAinda não há avaliações
- Apuntes de Patología BucalDocumento17 páginasApuntes de Patología BucalGeny RascónAinda não há avaliações
- Control de PlacaDocumento35 páginasControl de PlacaFabiola Elizabeth Cuevas MonsalveAinda não há avaliações
- CTZDocumento6 páginasCTZJorge Alberto NoguezAinda não há avaliações
- Aparato Disyuntor HiraxDocumento12 páginasAparato Disyuntor HiraxFernando Gutiérrez RamosAinda não há avaliações
- Erupcion DentariaDocumento12 páginasErupcion DentariaMickael Phill PiatAinda não há avaliações
- OrtopediaDocumento29 páginasOrtopediaElizabeth Castro GomezAinda não há avaliações
- Hipomineralización Incisivo MolarDocumento3 páginasHipomineralización Incisivo MolarMana V.Ainda não há avaliações
- Fracturas DentoalveolaresDocumento0 páginaFracturas DentoalveolaresMarisha CastroAinda não há avaliações
- Quiste NasopalatinoDocumento5 páginasQuiste NasopalatinoAndrea BellmuntAinda não há avaliações
- Maloclusion Clase IIDocumento4 páginasMaloclusion Clase IIAndres Felipe Cuartas UrreaAinda não há avaliações
- Quiste Residual y Caso ClínicoDocumento7 páginasQuiste Residual y Caso ClínicoMelanie PereiraAinda não há avaliações
- Instrumental de Endodoncia, Odontologia, Especialidad de EndodonciaDocumento39 páginasInstrumental de Endodoncia, Odontologia, Especialidad de EndodonciaAmy Hernández Guzmán100% (1)
- Tecnicas de AnestesiaDocumento18 páginasTecnicas de AnestesiaDaniel Suarez NatividadAinda não há avaliações
- Principios de Crecimiento MaxilofacialDocumento20 páginasPrincipios de Crecimiento MaxilofacialRicardo Cárdenas100% (2)
- Prevención de Impactación de CaninosDocumento56 páginasPrevención de Impactación de Caninosposgrado ortodoncia 2021Ainda não há avaliações
- PDF 20221015 000334 0000Documento37 páginasPDF 20221015 000334 0000Carlos A MartinezAinda não há avaliações
- Anomalias Dentarias en InfantilDocumento7 páginasAnomalias Dentarias en InfantilJORGE VILLANUEVA ARELLANESAinda não há avaliações
- Desarrollo EmbrionarioDocumento7 páginasDesarrollo EmbrionarioYessica JimenezAinda não há avaliações
- Cuestionario ORTODONCIADocumento10 páginasCuestionario ORTODONCIAVal EstefaniaAinda não há avaliações
- Trabajo 7 - OrtodonciaDocumento4 páginasTrabajo 7 - OrtodonciaThaylor JulcaAinda não há avaliações
- Atención en Salud Oral Del Paciente HemofílicoDocumento13 páginasAtención en Salud Oral Del Paciente HemofílicoEmel Pedrozo VásquezAinda não há avaliações
- Complejo Dentino-Pulpar - Pulpa DentalDocumento35 páginasComplejo Dentino-Pulpar - Pulpa DentalEnyha Vázquez MoraAinda não há avaliações
- Mini ImplantesDocumento3 páginasMini ImplantesASIA LOVER100% (1)
- Cuidados en salud bucal para personas con discapacidad sensorialNo EverandCuidados en salud bucal para personas con discapacidad sensorialAinda não há avaliações
- Arco Lingual Modificado para Verticalizar Molares VLDocumento5 páginasArco Lingual Modificado para Verticalizar Molares VLDenise RodsevichAinda não há avaliações
- Riesgos DesastresDocumento1 páginaRiesgos DesastresMilton David Rios SerratoAinda não há avaliações
- AdministraciónDocumento22 páginasAdministraciónMilton David Rios SerratoAinda não há avaliações
- Artritis ReumatoideDocumento2 páginasArtritis ReumatoideMilton David Rios SerratoAinda não há avaliações
- Analgesia Multimodal para El Control Del Dolor PostoperatorioDocumento2 páginasAnalgesia Multimodal para El Control Del Dolor PostoperatorioMilton David Rios SerratoAinda não há avaliações
- Analisis Funcional Sistema EstomatognaticoDocumento14 páginasAnalisis Funcional Sistema EstomatognaticoMilton David Rios SerratoAinda não há avaliações
- Diferencia Entre Dientes Temporales y PermanentesDocumento5 páginasDiferencia Entre Dientes Temporales y PermanentesMilton David Rios SerratoAinda não há avaliações
- CarnetDocumento1 páginaCarnetMilton David Rios SerratoAinda não há avaliações
- Anestesia Final 1Documento15 páginasAnestesia Final 1Milton David Rios SerratoAinda não há avaliações
- Certifica Do Libre Ta MilitarDocumento1 páginaCertifica Do Libre Ta MilitarMilton David Rios SerratoAinda não há avaliações
- LIbro 1 (Primera Parte) Dr. SatoDocumento5 páginasLIbro 1 (Primera Parte) Dr. SatoMilton David Rios SerratoAinda não há avaliações
- Antecedentes HistóricosDocumento19 páginasAntecedentes HistóricosMilton David Rios SerratoAinda não há avaliações
- ArgumentacionDocumento19 páginasArgumentacionMishelle Gabriela Tapia ZegarraAinda não há avaliações
- STO Version Español PDFDocumento99 páginasSTO Version Español PDFMilton David Rios Serrato100% (1)
- Resumen Matrícula MercantilDocumento2 páginasResumen Matrícula MercantilMilton David Rios SerratoAinda não há avaliações
- Alteraciones DentomaxilaresDocumento10 páginasAlteraciones DentomaxilaresjharmandoAinda não há avaliações
- Atm NeuromuscularDocumento58 páginasAtm NeuromuscularMilton David Rios Serrato50% (2)
- Un Espacio Entre NosotrosDocumento1 páginaUn Espacio Entre NosotrosMilton David Rios SerratoAinda não há avaliações
- Articulo 9 - Milton Rios - En.esDocumento10 páginasArticulo 9 - Milton Rios - En.esMilton David Rios SerratoAinda não há avaliações
- Activador Rígido Klammt para Clase IIDocumento1 páginaActivador Rígido Klammt para Clase IIMilton David Rios SerratoAinda não há avaliações
- Adhesion Disco Reporte CasoDocumento4 páginasAdhesion Disco Reporte CasoMilton David Rios SerratoAinda não há avaliações
- Activador Rígido Klammt para Clase IIDocumento1 páginaActivador Rígido Klammt para Clase IIMilton David Rios SerratoAinda não há avaliações
- Articulo 9 - Milton Rios - En.esDocumento10 páginasArticulo 9 - Milton Rios - En.esMilton David Rios SerratoAinda não há avaliações
- Alteraciones DentomaxilaresDocumento10 páginasAlteraciones DentomaxilaresjharmandoAinda não há avaliações
- Alteraciones DentomaxilaresDocumento10 páginasAlteraciones DentomaxilaresjharmandoAinda não há avaliações
- El Sto InicialDocumento102 páginasEl Sto InicialMilton David Rios SerratoAinda não há avaliações
- Molar Uprighting Simplified - En.esDocumento4 páginasMolar Uprighting Simplified - En.esMilton David Rios SerratoAinda não há avaliações
- Vertical MolarDocumento18 páginasVertical MolarMilton David Rios Serrato100% (2)
- Active and Passive Self-Ligation - A Myth - .En - EsDocumento7 páginasActive and Passive Self-Ligation - A Myth - .En - EsMilton David Rios SerratoAinda não há avaliações
- ForsuscasoclinicoDocumento14 páginasForsuscasoclinicoMilton David Rios SerratoAinda não há avaliações
- 4 Tipos de Ansas para Verticalizar PDFDocumento5 páginas4 Tipos de Ansas para Verticalizar PDFMilton David Rios SerratoAinda não há avaliações
- PANCREATITISDocumento26 páginasPANCREATITISGuileAstu UrAinda não há avaliações
- Trastorno Del SueñoDocumento4 páginasTrastorno Del SueñoValdo CruzAinda não há avaliações
- L TC 514 Simbologia CivilDocumento14 páginasL TC 514 Simbologia CivilEnid MunozAinda não há avaliações
- Aprende Haciendo 03 OrganizaciondedatosDocumento4 páginasAprende Haciendo 03 OrganizaciondedatosTierra OrgánicaAinda não há avaliações
- Reglamento de Gestión Urbana para El Municipio de Chapala 2020Documento20 páginasReglamento de Gestión Urbana para El Municipio de Chapala 2020Lea pinedaAinda não há avaliações
- Resolución 7 de Abril de 2005Documento6 páginasResolución 7 de Abril de 2005Lucía Matellán FernándezAinda não há avaliações
- CURSO ESTIMACION DE COSTOS 1.ppt (Autoguardado)Documento36 páginasCURSO ESTIMACION DE COSTOS 1.ppt (Autoguardado)Marg3107Ainda não há avaliações
- RESISTENCIA DE MATERIALES Semana 4 NocDocumento31 páginasRESISTENCIA DE MATERIALES Semana 4 NocFrancisco OsorioAinda não há avaliações
- Semana 1 y 2 ENERO Media General y TécnicaDocumento30 páginasSemana 1 y 2 ENERO Media General y Técnicacruzmsotillor100% (1)
- Foro 5 Salcedo Reátegui José RobertoDocumento2 páginasForo 5 Salcedo Reátegui José RobertoJoséSalcedoReáteguiAinda não há avaliações
- Resumen de Esquilache-Molina 1988Documento3 páginasResumen de Esquilache-Molina 1988PRILK2011Ainda não há avaliações
- Informe Introduccion 6 y 7Documento7 páginasInforme Introduccion 6 y 7Camily PlúasAinda não há avaliações
- Barrios de Verdad Kupini IIDocumento49 páginasBarrios de Verdad Kupini IIGobierno Autónomo Municipal de La Paz100% (2)
- Clausulado Seguro de Casco y Maquinaria (Navegación) 2019Documento34 páginasClausulado Seguro de Casco y Maquinaria (Navegación) 2019Maira DuranAinda não há avaliações
- Calendario Felicidad en El Trabajo5Documento18 páginasCalendario Felicidad en El Trabajo5ManuelAinda não há avaliações
- Wa0016.Documento24 páginasWa0016.Loretta krepchukAinda não há avaliações
- Fundamentos Python2Documento5 páginasFundamentos Python2Olga Marina Cuero RivasAinda não há avaliações
- MercadotecniaDocumento24 páginasMercadotecniaYeimy RaxicAinda não há avaliações
- Valores Universales Triptico #Documento4 páginasValores Universales Triptico #Paola Dennise Zapote RangelAinda não há avaliações
- Trabajo de Grado Norma Ohsas 18001:2007 y El Decreto 1443 de 2014Documento137 páginasTrabajo de Grado Norma Ohsas 18001:2007 y El Decreto 1443 de 2014YaMiLe PoSaDaAinda não há avaliações
- Historia de Vida DefinicionDocumento2 páginasHistoria de Vida Definicionlolito fernandezAinda não há avaliações
- Practica Dinamica N#2Documento8 páginasPractica Dinamica N#2JhosiitaVasquezAinda não há avaliações
- FichasDocumento30 páginasFichasIngrid Kimberly100% (1)
- El TonderoDocumento3 páginasEl TonderosergioyoveraAinda não há avaliações
- Instrucciones y Rubrica - Ejercicio Informacion Garifunas - Actividad 1Documento4 páginasInstrucciones y Rubrica - Ejercicio Informacion Garifunas - Actividad 1JOSUE DAVID BARDALES JULEAinda não há avaliações
- Mecanismos CoordinacionDocumento17 páginasMecanismos Coordinacionyoni hernan bances lalupuAinda não há avaliações
- Trabajo Escala de MohsDocumento12 páginasTrabajo Escala de MohsMarilyn Lisbeth Guerrero SalazarAinda não há avaliações
- Antropología Aplicada A La Medicina Resumen de La Unidad 1Documento4 páginasAntropología Aplicada A La Medicina Resumen de La Unidad 1Adriana CarrionAinda não há avaliações
- Escuela Secundaria Técnica 135 "Tlacaelel" 15DST0144G Zona Escolar Xxi Sector Viii Ciclo Escolar 2022-2023Documento2 páginasEscuela Secundaria Técnica 135 "Tlacaelel" 15DST0144G Zona Escolar Xxi Sector Viii Ciclo Escolar 2022-2023Gerardo FruteroAinda não há avaliações